There has been significant progress in limb salvage in patients with peripheral artery disease (PAD) and critical limb ischaemia (CLI) over the past two decades. These advancements have been promoted by the increased knowledge and understanding of the disease processes as well as the refinement in the interventions and enhanced patient care after revascularisation. Writing for Vascular News, Bauer E Sumpio introduces a new tool for assessing foot perfusion—hyperspectral imaging—and explains how it adds to the vascular specialists’ armamentarium.

Invasive and/or non-invasive angiography remains the gold standard for visualising the atherosclerotic lesions but newer technology is now emerging as vascular specialists shift their focus from a macro limb perspective to a more regional foot perspective. Among the current and emerging regional perfusion imaging modalities is hyperspectral imaging (HSI) using visible light which may help delineate regional foot perfusion for guiding directed revascularisation therapy of PAD/CLI.
The most important factor for determining the healing potential of a pedal wound is the degree of perfusion to the affected foot segment. The classic pathway for assessment involves history taking, physical examination, and review of both physiological markers and anatomical imaging obtained through non-invasive imaging.1 However, due to the persistent rate of limb loss despite revascularisation via the “best vessel” approach, there has been increasing interest in performing targeted reperfusion interventions to improve rates of limb salvage and decrease rates of secondary complications. The angiosome concept, was introduced by Taylor and Palmer more than 25 years ago, and extended to the foot by Attinger.2,3 Since then there have been various studies comparing outcomes for both open bypass and endovascular interventions using angiosome-based revascularisation (direct) versus non-angiosome-based revascularisation (indirect).4 With the growing interests in targeted revascularisation for regional areas of lower limb ischaemia, new modalities are now evaluating micro-perfusion in the lower extremity guided by the angiosome model.
Hyperspectral imaging
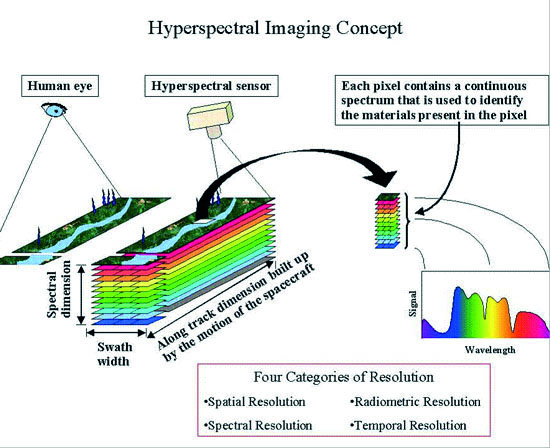
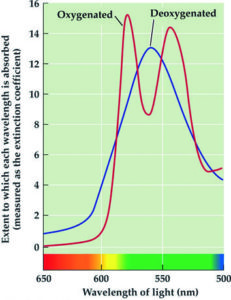
HSI utilises scanning spectroscopy to construct spatial maps for tissue oxygenation using wavelengths (between 500–700 nanometres [nm]) of visual light (Figure 1). These wavelengths penetrate to 1–4mm below the skin to the subpapillary plexus. The subcutaneous arteries form a network in the subpapillary plexus and supply the skin with blood. By combining digital imaging with conventional spectroscopy, targeted wavelengths for the absorption profile for oxyhaemoglobin and deoxyhaemoglobin can be identified and measured.
Chin et al5 reported differences in the tissue oxygenation of patients with PAD along angiosome regions of the foot. They identified significant differences in deoxyhaemoglobin at the plantar angiosomes, which encompasses the plantar metatarsal, plantar arch, and plantar heel. The level of deoxyhaemoglobin in these angiosomes was found to be decreased in patients with PAD compared to non-PAD patients. Nuovong et al6 performed a prospective study, demonstrating that HSI is predictive of ulcer healing in diabetic patients with foot ulcers. They reported higher oxyhaemoglobin levels in the 85% of diabetic foot ulcers that healed vs. the 64% that did not heal. They concluded that HSI offers high sensitivity (86%) and specificity (88%) in determining healing potential.

Because the prognosis of ischaemic vascular disease is directly related to the functional perfusion level, rather than merely a vascular structure, functional perfusion imaging is superior to structural vascular imaging in guiding targeted therapy via the angiosome model (Figure 2). Compared to ankle brachial index (ABI) and pulmonary vascular pressure, HSI can deliver a finer assessment of perfusion in specific anatomic areas. This is accomplished through its anatomic oxygenation maps in contrast to the gross oxygenation used in ABIs. Its non-invasive nature is a major asset, as no patient contact is necessary to image the target area. The use of visual wavelengths of light can further protect patients from exposure to ionising radiation. Anatomic maps can be rendered with other modalities, however, HSI avoids the use of intravenous contrast agents, which often require more highly-trained personnel, elaborate examination areas, and supply storage facilities.

HSI may still remain vulnerable to weaknesses faced by other skin perfusion detectors such as TcPO2 and LDF. Inflammatory reactions, such as those induced by infection, could cloud the interpretation of measurements in with local hyperaemia exists. Target area positioning will also need to be standardised as the study by Chin et al5 suggested detectable changes to the veno-arteriolar reflex with ischaemia. Nonetheless, the study by Nuovong et al6 does demonstrate the feasibility of HSI to identify changes in skin microcirculation in diabetic patients. Furthermore, a recent prospective non-randomised single-centre controlled trial performed by Chiang et al on 294 patients demonstrated the reliability of HSI to TcPO2, ABI, skin temperature, and severity of PAD with good correlation and low inter-operator and intra-operator variability.7 The authors conclude that HSI may be useful as a screening tool in early-stage PAD. In addition, HSI has demonstrated an ability to show real-time perfusion of the angiosome for preoperative planning. This technology can potentially evaluate the level of reperfusion after an intervention to monitor success or failure after index procedure.
With the knowledge that the prognosis of PAD and CLI is closely correlated to the functional perfusion level of the affected extremity rather than the macro-vascular structure, regional foot perfusion imaging may predict wound healing success in addition to becoming a dependable surveillance tool. The clinical evaluation of the angiosome model will only be truly realised if a proper imaging system is in place that is non-invasive, fast, and safe and can easily delineate wound topography to guide directed revascularisation therapy. With increasing interest and continued refinement in our understanding of PAD/CLI, the field of vascular surgery moves towards achieving a significant reduction in persistent ulceration and a decreasing the rate of complications after revascularisation for our patients. To accomplish this we must be willing to adopt new paradigms and techniques in the treatment of this complex disease process. The implementation of these newer modalities as part of our routine clinical evaluation appears increasingly closer as each individual technology is optimised and we understand how to better utilise them effectively in conjunction with clinical judgment.
The adaption of the angiosome model as well as utilising perfusion-based imaging studies allows the vascular specialists to refine their understanding of the disease process in CLI while enhancing therapeutic modalities, clinical decision-making, and improving outcomes after revascularisation interventions.
Bauer E Sumpio is a Professor of Surgery, Radiology and Medicine, Yale University School of Medicine, New Haven, USA. He is on the Scientific Advisory Board of HyperMed Imaging, Inc
References
- Benitez E, Sumpi BJ, Chin J, Sumpio BE. Semin Vasc Surg 2014; 27 (1):3–15.
- Attinger CE, Evans KK, Bulan E, et al. Plastic and Reconstructive Surgery 2006; 117 (7 Suppl):261S–293S.
- Clemens MW, Attinger CE. Foot Ankle Clin 2010; 15 (3):439–464.
- Sumpio BE, Forsythe RO, Ziegler KR, et al. J Vasc Surg 2013; 58 (3):814–826.
- Chin JA, Wang EC, Kibbe MR. J Vasc Surg 2011; 54 (6):1679–1688.
- Nouvong A, Hoogwerf B, Mohler E, et al. Diabetes care 2009; 32 (11):2056–2061.
- Chiang, N, Jain J, Sleigh J, Vasudevan T. J Vasc Surg 2017; 66(4):1192–1201.












Has the new tool a registration for Europe?