This article forms part of an educational supplement sponsored by Shockwave Medical. Explore the full Compliance is Key series here.

Bella Huasen (Lancashire Teaching Hospitals NHS Foundation Trust, Preston, UK) outlines a recent femoropopliteal occlusion case, during which Shockwave Intravascular Lithotripsy (IVL; Shockwave Medical) proved to be an effective vessel preparation strategy in this ‘no-stent zone’.
There are no signs of atherosclerotic disease regression internationally, with an increasing number of chronic limb-threatening ischaemia (CLTI) patients presenting with heavily calcified disease and ulcerations. Whilst healthcare authorities work on prevention strategies, we as endovascular clinicians must work hard on ‘cures’ to avoid amputation. In our trust, cases are discussed at the CLTI multidisciplinary team meeting every week, and those with calcific disease are listed for endovascular intervention with Shockwave IVL. IVL is helping fight against calcium by increasing vessel wall compliance, thus minimising significant dissection and procedural complications and resulting in acute procedural success with a significantly reduced need for stenting. In our CLTI algorithm, IVL is not classed as an alternative but as an adjunctive therapy to our current treatment pathway by providing consistent vessel preparation for a definitive treatment strategy. This is a simple and effective tool, often used as part of day-case work, and so the learning curve is short.
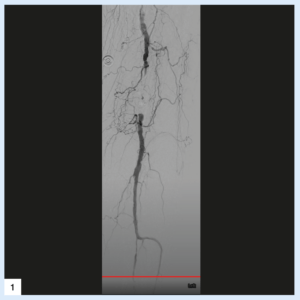
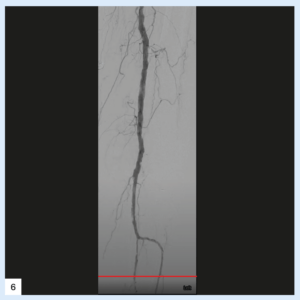
We present an 85-year-old female with multiple comorbidities including hypertension, diabetes mellitus type 2, and cardiac disease, who came to our care with Rutherford 5 CLTI involving painful ulcers affecting the second and third toe, limiting mobility and self-confidence. Computed tomography angiography (CTA) imaging confirmed an occlusive lesion of the distal superficial femoral artery (SFA) into the proximal popliteal artery (POPA) with little flow into the foot. We were keen to avoid treatment that would require stent insertion alone due to the associated risk of stent failure in this region, where high pressure and mechanical dynamics in limb flexion create deformations and the literature suggests many existing stent designs are not yet successfully able to withstand the repetitive movement that impacts artery-stent combination.
The procedure was performed as a day case. On-table Doppler ultrasound confirmed the CTA findings. Subcutaneous 1% lidocaine local anaesthetic was infiltrated under ultrasound guidance followed by puncture of the common femoral artery in antegrade access using the Seldinger technique. Initially, a 4Fr sheath was inserted. Angiogram confirmed occlusive disease of the distal SFA-POPA. A long, 7Fr Advantage sheath (Terumo) and 0.014” Advantage track wire (Terumo) were used to cross the occlusion. This was followed by a 7x60mm Shockwave M5+ IVL catheter (Shockwave Medical), which was used across the calcified length of the lesion using all the 300 pulses available on the catheter. It is important to up size, to obtain maximum benefits. Focus was made to cover the entire lesion area and cross cover the entry-exit site of subintimal spaces. Successful vessel preparation was achieved with low residual stenosis and without dissection or distal embolisation. Treatment of the target lesion was concluded using a 7mm sirolimus balloon (Selution, MedAlliance) which was inflated for three minutes. Finally, the crural arteries were treated using 1.5–2.0–2.5mm tapered balloons. A 6Fr Angioseal (Terumo) was used for haemostasis. There were no immediate or late complications. The patient was on dual antiplatelet therapy for three months. There was no further intervention in an 18-month period with almost complete resolution of the ulcers.
Case images


Bella Huasen is an endovascular and interventional radiology consultant at Lancashire Teaching Hospitals NHS Foundation Trust in Preston, UK.











