
The incidence of ruptured abdominal aortic aneurysm (AAA) and associated mortality has decreased over the past 20 years in Sweden, indicating that altered smoking patterns have had an impact on overall AAA prevalence and aneurysm rupture and that endovascular aneurysm repair (EVAR) has helped to improve overall survival. However, more attention needs to be placed on improving the outcome of ruptured AAA in women.
These are the findings from a nationwide assessment of the epidemiology of ruptured AAA over 20 years, which point to increasing surgical rate and improved survival of ruptured AAA patients. The results of the assessment were presented by Kim Gunnarsson (Uppsala University, Uppsala, Sweden) at the European Society for Vascular Surgery’s annual meeting (ESVS; 25–28 September, Valencia, Spain).
According to Gunnarsson, the epidemiology of ruptured AAA, as well as the clinical management, has changed over recent decades due to a number of factors, including changes in smoking habits, cardiovascular disease management, the introduction of EVAR, as well as screening for aortic aneurysms. Most assessments of ruptured AAA epidemiology, he pointed out, focus on the patients undergoing surgical intervention, however, historical cohorts indicate that only half of the patients with ruptured AAA are hospitalised and only a selection of those patients undergo surgery.
In this population-based study, Gunnarsson and colleagues aimed to investigate the modern epidemiology of ruptured AAA. The study includes an assessment of the total incidence of ruptured AAA, including ruptures resulting in death prior to hospitalisation, the proportion of ruptured AAA patients presenting alive to hospital and operated on and the total mortality rate for ruptured AAA.
 Thanks to a unique personal identification number for each individual in Sweden, data captured from 1994–2013 in three national registries could be included in this study: the National Patient Registry, capturing all hospital episodes with a diagnosis of AAA; the Cause of Death Registry; and the Swedish Vascular Registry, including all operations performed for ruptured AAA. The investigators captured all ruptured AAA occurring in individuals above 50 years of age in all three registries. The total cohort included 18,726 cases, of which 74% were men, and 34% of the men and 53% of the women were above 80 years of age.
Thanks to a unique personal identification number for each individual in Sweden, data captured from 1994–2013 in three national registries could be included in this study: the National Patient Registry, capturing all hospital episodes with a diagnosis of AAA; the Cause of Death Registry; and the Swedish Vascular Registry, including all operations performed for ruptured AAA. The investigators captured all ruptured AAA occurring in individuals above 50 years of age in all three registries. The total cohort included 18,726 cases, of which 74% were men, and 34% of the men and 53% of the women were above 80 years of age.
To evaluate the change in the incidence of ruptured AAA, Gunnarsson and colleagues used a linear regression model which described the incidence per 100,000 population above the age of 50 years. They found that among men the decrease was 45%, but in women, on the other hand, there was no change over time. Further, the research showed that the proportion of ruptured AAA patients that presented to hospitals alive and therefore having a chance to be operated on increased over time. In men, there was an increase from 65–72% over the two decades, and in women there was an increase from 51–58%.
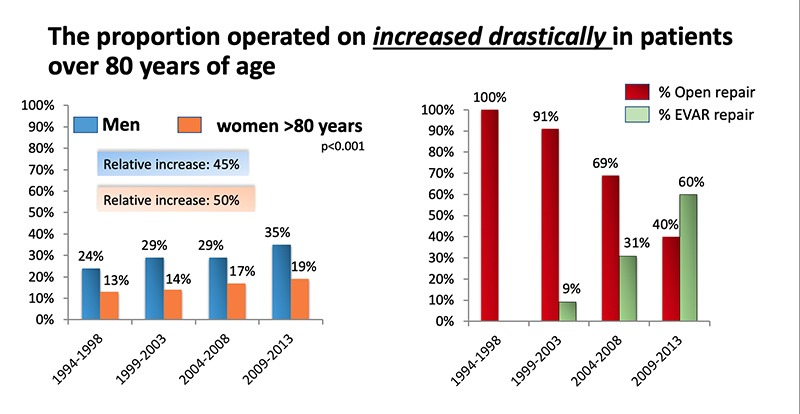
In this cohort, Gunnarsson reported, there was a significant amount of patients over 80 years of age, and they observed a “drastic” increase in the number of patients in this group being operated on. In men, there was a relative increase of 45% and in women a relative increase of 50%. This increase, he pointed out, had an association with an increased use of EVAR for ruptured AAA. The first use of EVAR for ruptured AAA was recorded in 1995, and from 2009–2013, 60% of all patients over 80 years of age who underwent surgery for a ruptured AAA were treated with EVAR.
When analysing the mortality rate, the study found a decrease in overall ruptured AAA-related mortality, but for women, even though there was a slight decrease over time, between 2009 and 2013, the rate of mortality was still 82%, compared to 89% from 1994–1998, a relative decrease of 7% over 20 years. In men, the rupture-related mortality decreased from 76% in the 1994–1998 period to 65% in the 2009–2013 period, a relative decrease of 15%.
The strengths of this study, Gunnarsson said, lie in the fact that it is a national population-based study, including all ruptured AAA cases from three cross-linked registries. The limitations, he admitted, are the risk of coding errors and an autopsy rate of just 10%, resulting in the risk for misdiagnosis of sudden deaths. However, he said, “as the autopsy rate is stable, one can assume that the error rate related to miscoding was also stable over time”.
“In conclusion, the total incidence and mortality due to ruptured AAA has decreased over the past two decades in Sweden. There is also an increasing proportion of patients with ruptured AAA presenting to hospital and being operated on with an improved survival. And women have a very high mortality rate in ruptured AAA compared to men,” Gunnarsson said.
The interpretation of these findings, he added, suggest that the reduction in prevalence of AAA, much thanks to altered smoking patterns, is mirrored in rupture incidence, and EVAR has resulted in a more active intervention in elderly patients with ruptured AAA, thus improving overall ruptured AAA survival. Finally, Gunnarsson noted that this study indicates that there is a need for focused efforts to improve the outcome of ruptured AAA in women.











