It is imperative that every medical institution has an interdisciplinary CLI team, argues Jihad Mustapha. Here, he exhorts the benefits of working in such a multidisciplinary team, and outlines how the circle of care concept can be applied to reduce rates of unnecessary major amputation.
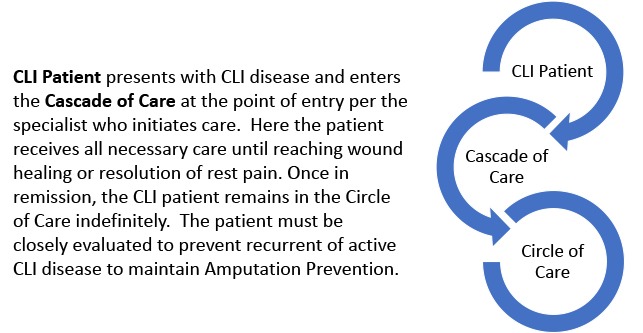
The most effective critical limb ischaemia (CLI) multidisciplinary team structure is comprised of multiple layers or groups of providers from a variety of areas, including surgical and endovascular revascularisation, podiatry, wound care, endocrinology, primary care, orthopaedics, cardiology, infectious disease and physical medicine. The action of each group is reactive to the immediate need of the CLI patient. The course of action in the treatment cascade is not linear; instead, it is both repetitive and reactive. To transform the potentially catastrophic event of a CLI diagnosis into a patient with a successful outcome, the team must act in harmony and initiate the reactive cycle of therapy when a CLI patient receives treatment at the level that is most critical at any single point in time (Figure 1). A provider will refer the CLI patient to the next most critical continuum for the secondary issue to be addressed (cascade of care). The CLI team must always be aware of and acknowledge that the CLI patient’s therapy is not conclusive, and that the chance of recurrent disease is high. Therefore, heightened awareness and strict follow-up evaluation are required. Once a recurrent CLI event is discovered, the repetitive cycle must be initiated. For a patient with active CLI disease, there should never be a period of time where no form of therapy is being delivered. The average time it takes for a CLI patient to receive any type of first treatment or diagnostic testing has been reported to be nine days. This is unacceptable. Too much can happen in nine days to result in a poor outcome for a CLI patient. Therefore, the repetitive phase must be initiated as early as possible.
Any member of the CLI team can and should trigger the repetitive treatment cascade in the presence of:
- Recurrent rest pain
- Absent doppler pulse
- Occluded target vessel and lack of progression of wound healing
- Regression of wound healing
- Infection or sepsis. Note: Amputation is not always the answer here. Revascularisation and intravenous antibiotics must be tried first, unless the patient is in shock and the limb is not salvageable. Only then should amputation be performed without an attempt at revascularisation.
Once a CLI patient has been treated and has reached a stable form of the disease, such as wound healing, rest pain resolution and/or return to activity, the preventive phase of CLI therapy (in the circle of care) should be initiated by the CLI team. The CLI team members must each provide their recommended medical treatment based on their specialty. Most importantly, the circle of care (preventive phase) should never be stopped. In fact, prevention should be started in the pre-CLI phase for patients who are Rutherford 1–3. Any form of peripheral arterial disease (PAD) should be preventively treated as early as possible to prevent the catastrophic outcomes that we know can happen to those patients that reach the CLI phase. Hence, there is an extreme need for a multidisciplinary CLI team to exist in every institution in the USA and around the globe.

CLI centres are a new concept, and have adopted the strategies discussed above. The success of any CLI centre is dependent upon the harmony of the members of the multidisciplinary CLI team. CLI centres’ outcomes have been shown to produce excellent outcomes with impressive reductions in major amputation.1,2 The future of effective CLI therapy lives in a cohesive and functional multidisciplinary team.
Jihad A Mustapha is the associate clinical professor of Medicine at Michigan State University COM, E Lansing, USA. He is also the CEO of Advanced Cardiac and Vascular Centers for Amputation Prevention, Grand Rapids, USA.
References
1. Mustapha JA, Saab FA, Diaz-Sandoval LJ, Beasley R, McGoff T, Finton S, Heaney C, Adams G. The Peripheral RegIstry of Endovascular Clinical OutcoMEs (The PRIME Registry): Interim Analysis of the First 328 Subjects With Critical Limb Ischemia. Vascular Disease Management. 2017;14(3): E55-67.
2. Raymond Dattilo, Alexandra Dattilo, Shawn Colby. Outcomes of Patients Treated for Critical Limb Ischemia in an Outpatient Endovascular Center. Vascular Disease Management 2018;15(6):E49-E52.










