
First revealed at the International Symposium on the Diabetic Foot (22–25 June 2019, The Hague, The Netherlands), new guidelines from the International Working Group on the Diabetic Foot (IWGDF) have updated recommendations for the practice of diabetic foot care and treatment. This article overviews the latest approaches to offloading and considers the future of this treatment option for patients with diabetic foot wounds.
Peripheral neuropathy leads to changes in gait, foot deformity and soft tissue, all of which can further elevate mechanical stress.1–3 Thus, the combination of loss of protective sensation, and elevated mechanical stress, leads to tissue damage and the development of a diabetic foot ulcer (DFU).4
Once a DFU forms, healing is chronically delayed if the area is not effectively offloaded.4,5 Local wound management, infection management, revascularisation, and pressure offloading are all required, but offloading is arguably the most important of these interventions.6 Sadly, unhealed diabetic foot ulcers are a prelude to 84% of lower extremity amputations,1 so it is important to heal ulcers quickly and keep them healed.7
The IWGDF presents their own review of the literature with expert panel members to suggest new best practice guidelines, which are devised using a series of clinical questions and critically important outcomes to conduct a systematic review of the medical-scientific literature.
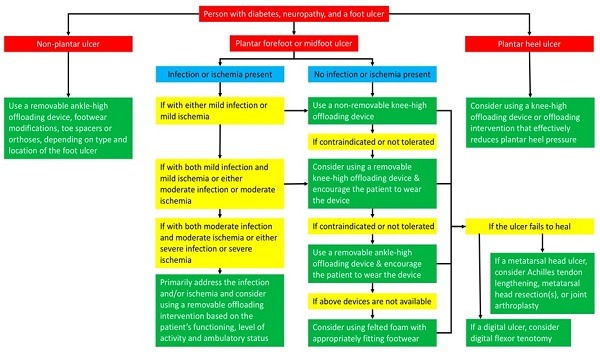
Recent guidelines on offloading focus on the management of neuropathic foot ulcers, with the prevention of foot ulcers now covered in the updated 2019 IWGDF prevention guideline.8 The new guidelines follow a friendlier format where possible, so they can outline the following, as shown in Figure 1 (below):
- The first-, second-, third- and fourth-choice of offloading treatment to heal a neuropathic plantar forefoot or midfoot ulcer.
- Added one new recommendation on considerations for choosing between either a total contact cast or non-removable knee-high walker.
- Added three new recommendations on offloading treatments for people with neuropathic plantar forefoot ulcers that are complicated by infection or ischaemia.
- Added a new recommendation on offloading treatments for people with neuropathic plantar heel ulcers.
In total, nine recommendations were produced in 2019, but only four were graded strong by the strength of recommendation, and high to moderate depending on the quality of evidence:
- A non-removable knee-high offloading device is the first-choice of offloading treatment. Strong; High.
- The use of a removable knee-high and removable ankle-high offloading device is to be considered as the second- and third-choice offloading treatment, respectively, if contraindications or patient intolerance to non-removable offloading exist. Strong; Moderate.
- In a person with diabetes and a neuropathic plantar forefoot or midfoot ulcer, do not use, and instruct the patient not to use, conventional or standard therapeutic footwear as offloading treatment to promote healing of the ulcer, unless none of the above-mentioned offloading devices are available. Strong; Moderate.
- In a person with diabetes and a non-plantar foot ulcer, use a removable ankle-high offloading device, footwear modifications, toe spacers, or orthoses, depending on the type and location of the foot ulcer, to promote healing of the ulcer. Strong; Low.
Since the last guidelines, total contact casting (TCC) is no longer the only treatment to effectively heal plantar forefoot ulcers. Prefabricated removable knee-high walkers that are rendered non-removable are thought to be beneficial due to more evidence being established in the last four years.
Even so, it has been emphasised that there is a need to measure factors impacting on mechanical stress levels that lead to different healing outcomes, which include:
- Plantar pressure,
- Shear stress,
- Weight-bearing activity that includes steps and standing duration,
- Adherence to using offloading devices.
A lack of standardisation leads to technical difficulties in comparing modalities, and there is still little data available on the value of offloading in healing plantar foot ulcers complicated by infection or ischaemia, rearfoot ulcers, or non-plantar ulcers.
Thereafter, recommendations become less defined, with lower levels of evidence and quality for their use. Medical treatments are only described with weak evidence. However, if nonsurgical offloading fails, the guidelines only consider surgical offloading interventions for healing metatarsal head and digital ulcers.
Surgical interventions
Surgical offloading has primarily been applied to heal foot ulcers in selected patients, typically where other nonsurgical offloading interventions have failed. The current IWGDF tends to include studies that have case control or higher-level evidence, which can mitigate the majority of surgical studies.
The treatments identified in the current IWDGF include tendon procedures such as toe flexor tenotomy and achilles tendon release, predominantly for pressure release. However, we are now seeing other surgical techniques and modalities used in offloading that were not described in the latest guidelines, supported by a number of systematic reviews/meta-analyses for surgical management of the diabetic foot.
Below, in order of invasiveness, we describe soft tissue procedures that could be conducted in the clinic, adjuvant modalities followed by bony off-loading in the form of exostectomy, and foot reconstruction that require a formal surgical process.
Tenotomy
This is a promising intervention in patients with hammertoes and recalcitrant digital ulcers who, in particular, fail with non-surgical treatment. The procedure works for a flexible hammertoe by decompressing the tight flexor tendon to allow the toe pulp to take weight again, and is performed in an outpatient setting, without the need for subsequent immobilisation.
However, the quality of the evidence for this recommendation was low; nevertheless, benefits of digital flexor tenotomy may outweigh the potential harm. The cost-effectiveness of this procedure has not been evaluated. Therefore, the strength of this recommendation was weak.
Achilles tendon release and metatarsal offloading
The question asked here was “will persons with diabetes, and a neuropathic plantar metatarsal head ulcer, consider using Achilles tendon lengthening, metatarsal head resection(s), or joint arthroplasty to promote healing of the ulcer, if non-surgical offloading treatment fails?”.
Again, surgical offloading techniques are only considered for those hard-to-heal plantar ulcers with non-surgical offloading interventions.9 These techniques change the foot structure and therefore provide a more permanent offloading solution for areas of elevated mechanical stress, even when the patient is not adherent to wearing an offloading device.
Surgical offloading potentially comes with an increased risk of complications compared with non-removable offloading devices alone, but have a higher efficacy of healing, shorter time-to-healing [by 24–43 days, p<0.05]. Also, early data from a recent low-quality controlled study of metatarsal head resection(s) found significant decreases in hospitalisations and infections compared to non-surgical offloading controls (p<0.05).10
Adjuvant local antibiotic loading
It is presumed that treating infection, coupled with surgical offloading and biofilm disruption, allows a non-healing ulcer to heal combined with offloading. Local antibiotic delivery can yield very high concentrations of antibiotics exclusively in targeted areas, which cannot be achieved by systemic therapy, despite it being useful in poorly perfused tissues.
This has been described with the current focus on biodegradable vehicles, such as cerement and stimulan. However, existing randomised controlled trials (RCTs) are only reporting the use of non-absorbable polymethylmethacrylate impregnated cement in diabetic foot infection.
Lipsky et al reported the randomised use or non-use of a gentamicin-collagen sponge, in addition to standard care, for moderately infected foot ulcers in 38 DFU patients,11 which showed significant rates of clinical cure and eradication of baseline pathogens. In general, rates of wound-healing and re-operation were good in the papers that were reviewed, but long-term follow-up is required.
In conclusion, the role of topical antibiotic agents in treating diabetic foot infections is limited, and current use of antibiotic bone void fillers to protect resection margins and allow healthy regeneration is still in its infancy. However, these processes may lead to early healing combined with off-loading.
Surgical exostectomy
In simple terms, this is the removal of material to achieve direct bony pressure offloading without providing definitive foot stabilisation. Current evidence suggests that medial exostectomy for offloading is a safe procedure. However, surgical decision making needs an understanding of osseous or bony instability.
This is particularly the case for the lateral column (or outer border of the foot), which involves the cuboid. Some have noted early radiographic changes leading to a need to repeat exostectomy for ulcers under the lateral column of the foot.12
Surgical reconstruction (stabilising foot shape for sustained plantar pressure reduction)
These techniques are used in limb salvage involving deformity correction, with the aim of keeping the foot flat to the floor, and plantigrade without pressure areas for ambulation. These patients suffer from deformity associated with Charcot neuroarthropathy and may have vascular insufficiency, requiring combined surgical treatment. The amputation risk is seven times higher for patients with an ulcer and 12 times higher for patients with Charcot and an ulcer, compared with Charcot alone.13
Surgical reconstruction either with external fixation (frames) or specialised implants, such as disease specific bolts and plates, shows much promise and results in single or own surgeon series are good, with low rates of re-ulceration and major complication, including amputations.14–19
This may be a process that is related to the level of medical care received after such surgeries, or ongoing follow-up within a multidisciplinary team. Even so, recent systematic reviews suggest limb salvage rates may in part be improving due to the continued development of superior implants. Therefore, Charcot foot reconstruction is likely to be a better alternative to lower limb amputation in selected cases.20
Summary
Sadly, the problem does not end with healing, and off-loading as Buss et al reveal;4 there must be a shift in emphasis, as healed foot ulcers frequently recur. This requires a collective refocus from acute offloading to long-term preventive offloading.
We still require standardisation of outcomes and measures of offloading, in addition to more high-quality evidence concerning surgical offloading procedures. This will help us to determine the impact of surgical interventions on the healing of both non-complicated and complicated foot ulcers.
Today, we are still learning more about harmonising and balancing the foot after surgery, as well as understanding resection margins of treatment to prevent ulceration.21 There is an increasing number of patients who now prefer to undergo limb salvage, fearing tissue loss more than life.21
Currently, there are no case-controlled studies or RCTs, but a number of meta-analyses confirm surgical efficacy from the results of what would be considered low-value studies.19 Formal case reporting in Charcot registries may be the next step then, as an RCT could have several ethical barriers that are quite difficult to overcome in this low-volume arena.
Conclusion
From the current update, it is clear that fixed offloading devices have superior efficacy, but heel ulcers remain difficult to treat. The gold standard is still TCC, and all other fixed, non-removable offloading devices are judged against it; the exact offloading capability of each is not fully known, so ongoing multidisciplinary team management is key.
Recurrence after healing is a problem; we heal ulcers as quickly as possible to avoid early amputation and tissue loss due to secondary infection. However, treatment strategies need to be progressive for long-term offloading, and we must consider surgical intervention to mechanically stabilise and harmonise the foot.
This may allow appropriate surgical decision making to avoid recurrence but requires an improvement in our understanding of anatomical foot reconstruction in these patients, defining a time point when surgery could protect against irretrievable tissue loss primarily, but also prevent re-ulceration and allow function to be retained.
Further evaluation has to be conducted using the concepts of value-based healthcare,23 where reduction in the episode of ulceration, and recurrence, will become important outcomes—we may well see these concepts in the next guidelines to reflect a new mindset in outcomes.
References:
- Lazzarini PA, Crews RT, Van Netten JJ, Bus SA, Fernando ME, Chadwick PJ, et al. Measuring Plantar Tissue Stress in People with Diabetic Peripheral Neuropathy: A Critical Concept in Diabetic Foot Management. Journal of Diabetes Science and Technology. 2019; 0(0):1932296819849092.
- Fernando ME, Crowther RG, Pappas E, Lazzarini PA, Cunningham M, Sangla KS, et al. Plantar pressure in diabetic peripheral neuropathy patients with active foot ulceration, previous ulceration and no history of ulceration: a meta- analysis of observational studies. Plos One. 2014; 9(6): e99050.
- Fernando M, Crowther R, Lazzarini P, Sangla K, Cunningham M, Buttner P, et al. Biomechanical characteristics of peripheral diabetic neuropathy: A systematic review and meta-analysis of findings from the gait cycle, muscle activity and dynamic barefoot plantar pressure. Clinical Biomechanics (Bristol, Avon). 2013; 28(8):831-45.
- Armstrong DG, Boulton AJM, Bus SA. Diabetic Foot Ulcers and Their Recurrence. New England Journal of Medicine. 2017; 376(24):2367-75.
- Bus SA, van Deursen RW, Armstrong DG, Lewis JEA, Caravaggi CF, Cavanagh PR, et al. Footwear and offloading interventions to prevent and heal foot ulcers and reduce plantar pressure in patients with diabetes: a systematic review. Diabetes/Metabolism Research and Reviews. 2016; 32:99-118.
- Schaper NC, Van Netten JJ, Apelqvist J, Lipsky BA, Bakker K, on behalf of the International Working Group on the Diabetic F. Prevention and management of foot problems in diabetes: A Summary Guidance for Daily Practice 2015, based on the IWGDF Guidance Documents. Diabetes/Metabolism Research and Reviews. 2016; 32:7-15.
- Reiber GE, Pecoraro RE, Koepsell TD. Risk factors for amputation in patients with diabetes mellitus. A case control study. Ann Intern Med. 1992;117(2):97–105.
- Bus SA, Lavery LA, Monteiro-Soares M, Rasmussen A, Raspovic A, Sacco ICN, et al. IWGDF Guideline on the prevention of foot ulcers in persons with diabetes. Diabetes/Metabolism Research & Reviews. 2019; in press.
- Bus SA, Valk GD, van Deursen RW, Armstrong DG, Caravaggi C, Hlavácek P, et al. The effectiveness of footwear and offloading interventions to prevent and heal foot ulcers and reduce plantar pressure in diabetes: a systematic review. Diabetes/Metabolism Research & Reviews. 2008; 24: S162-80.
- Motamedi AK, Ansari M. Comparison of Metatarsal Head Resection Versus Conservative Care in Treatment of Neuropathic Diabetic Foot Ulcers. J Foot Ankle Surg. 2017; 56(3):428-33.
- Lipsky BA, Kuss M, Edmonds M, Reyzelman A, Sigal F. Topical application of a gentamicin-collagen sponge combined with systemic antibiotic therapy for the treatment of diabetic foot infections of moderate severity: a randomized, controlled, multicenter clinical trial. J Am Podiatr Med Assoc. 2012; 102:223-232.
- Laurinaviciene R, Kirketerp-Moeller K, Holstein PE. Exostectomy for chronic midfoot plantar ulcer in Charcot deformity. J Wound Care. 2008; 17:53-55.
- Sohn MW, Stuck RM, Pinzur M, Lee TA, Budiman Mak E. Lower-Extremity Amputation Risk After Charcot Arthropathy and Diabetic Foot Ulcer. Diabetes Care. 2010 Jan; 33(1):98-100. doi: 10.2337/dc09-1497.
- Dayton P, Feilmeier M, Thompson M, Whitehouse P, Reimer RA. Comparison of Complications for Internal and External Fixation for Charcot Reconstruction: A Systematic Review. Foot Ankle Surg. 2015 Nov-Dec; 54(6):1072-5. doi: 10.1053/j. jfas.2015.06.003. Epub 2015 Jul 26.
- Lee DJ, Schaffer J, Chen T, Oh I. Internal Versus External Fixation of Charcot Midfoot Deformity Realignment. 2016 Jul 1;39(4): e595601. doi: 10.3928/01477447-20160526-11. Epub 2016 Jun 6.
- Emara KM, Ahmed Diab R, Amr Hemida M. Tibiocalcaneal fusion by retrograde intramedullary nailing in charcot neuroarthropathy. Foot (Edinb). 2018 Mar; 34:6-10. doi: 10.1016/j.foot.2017.11.003. Epub 2017 Nov 7.
- Wiewiorski M1, Yasui T, Miska M, Frigg A, Valderrabano V. Solid bolt fixation of the medial column in Charcot midfoot arthropathy. J Foot Ankle Surg. 2013 Jan-Feb;52(1):88-94. doi: 10.1053/j. jfas.2012.05.017. Epub 2012 Aug 28.
- Vasukutty*, H. Jawalkar, A. Anugraha, et al. Correction of ankle and hind foot deformity in Charcot neuroarthropathy using a retrograde hind foot nail—The Kings’ Experience. http://dx.doi. org/10.1016/j.fas.2017.04.014
- Shazadeh Safavi P, Jupiter DC, Panchbhavi V. A Systematic Review of Current Surgical Interventions for Charcot Neuroarthropathy of the Midfoot. J Foot Ankle Surg. 2017 Nov – Dec; 56(6):1249-1252. doi: 10.1053/j.jfas.2017.06.011. Epub 2017 Aug 1.
- Dayton P, Feilmeier M, Thompson M, Whitehouse P, Reimer RA. Comparison of Complications for Internal and External Fixation for Charcot Reconstruction: A Systematic Review.
- Suh YC, Kushida-Contreras BH, Suh HP, et al. Is Reconstruction Preserving the First Ray or First Two Rays Better Than Full Transmetatarsal Amputation in Diabetic Foot? Plast Reconstr Surg. 2019 Jan; 143(1):294-305. doi: 10.1097/ PRS.0000000000005122.
- Wukich DK, Sadoskas D, Vaudreuil NJ, Fourman M. Comparison of Diabetic Charcot Patients with and Without Foot Wounds. Foot Ankle Int. 2017 Feb; 38(2):140-148. doi: 10.1177/1071100716673985. Epub 2016 Oct 24.
- Porter ME, What Is Value in Health Care? N Engl J Med 2010; 363:2477-2481. DOI: 10.1056/ NEJMp1011024
Raju Ahluwalia is a full-time orthopaedic consultant foot and ankle surgeon at King’s College Hospital NHS Foundation Trust, London, UK, trained in London and Cambridge, and is undertaking advanced training at RNOH Stanmore and Oxford. He is an elected executive committee member of the Diabetic Foot Study Group of the European Association for the Study of Diabetes (EASD) and sits on the International Diabetic Foot Care Group.
Chris Manu is a consultant diabetologist and general medicine at King’s College Hospital NHS Foundation Trust and Bromley Healthcare, London, UK, with clinical and academic sub-speciality interest in the diabetic foot disease, and transformation lead for diabetic foot disease in south east London. He is a member of the International Diabetic Foot Care Group and part of the team developing the Fast Track Pathway.
Ines L Reichert completed a PhD in Fracture Healing and Bone Blood, and fellowships at St Michael’s Hospital, Toronto, Canada. She undertakes complex trauma and diabetic foot reconstruction. She has maintained an active interest in research and is a member of the British Orthopaedic Research Society. She also serves on the editorial board of Bone & Joint Research and is the orthopaedic and rheumatology research and development lead for clinical studies at King’s College Hospital NHS Foundation Trust, London, UK.
The authors would like to acknowledge Michael Edmonds in developing ideas and preparation of the manuscript.








