
Saphenous pulsation is the cyclical impulse of antegrade flow observed on colour duplex ultrasound after prolonged standing. It is a common observation in patients with saphenous reflux and is detected in the upper part of the great saphenous vein, remote from neighbouring arterial interference. Interest in pulsation has been renewed by its potential as a marker of severe chronic superficial venous insufficiency.
The sequence of colour flow changes in patients with saphenous reflux, from a position of elevation to non-weight bearing dependency. It commences with reflux (shown in red) throughout the cross-sectional area of the vein. This can last for up to, and possibly over, one minute. The reflux becomes less intense with time and finally disappears, last visible at the centre of the lumen. This is followed by a few seconds of no-flow visualised as a black lumen.
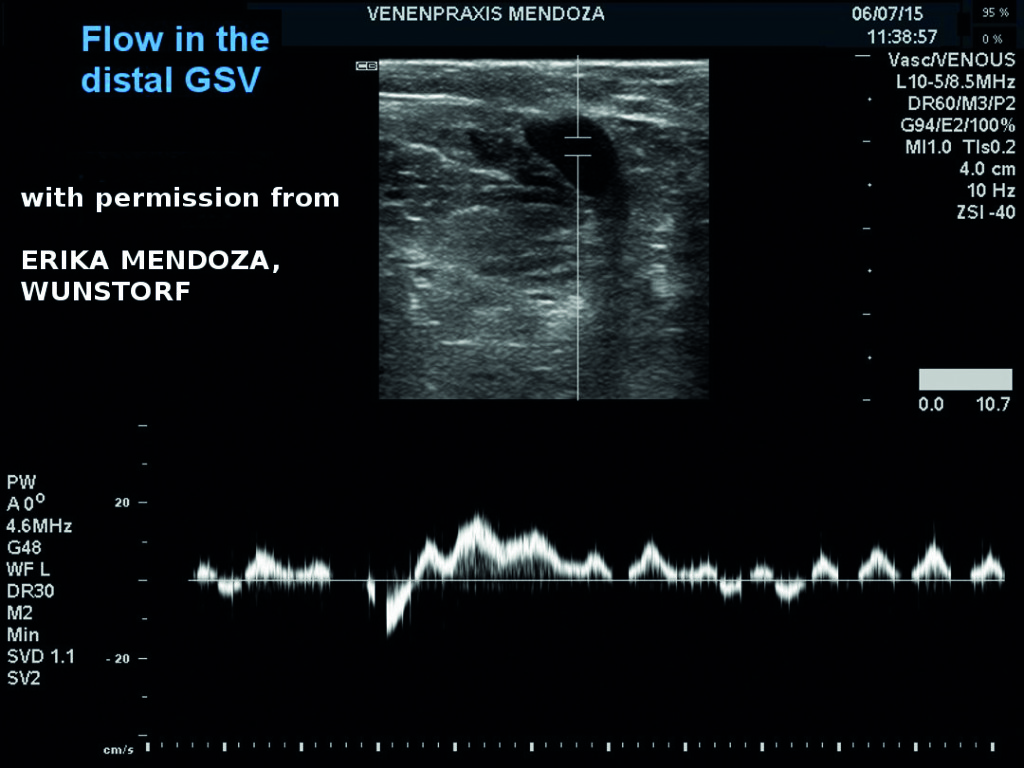
Eventually, impulses of antegrade flow (shown in blue) begin to appear at the centre of the lumen, spreading to fill the entire lumen over a background of black. The frequency may not be similar to the heart rate and could be as low as 22 cycles per minute. The saphenous pulsation is often irregular and of varying intensity. Slight movements at this stage, which include coughing or talking, result in breakthrough reflux (red).
Respiratory phasicity represents normal physiological flow in the deep leg veins of the thigh. It is synchronous with the respiratory cycle and becomes augmented during deep inspiration and exhalation. Respiratory movements may influence the saphenous pulsation and be responsible for its variable amplitude and irregular waveform. However, it is clear from the higher pulsation frequency that this is not the main driver of saphenous pulsation.
Our hypothesis is that saphenous pulsation represents a failing microcirculation where the arterial impulse is transmitted onto the superficial venous network. The exact pathophysiology of this vis-a-tergo (force from behind) is not known, but theories include a reduction in arterial resistance from venous hydrostatic back pressure or the opening up or development of arterio-venous communications or shunts. The irregular nature of saphenous pulsation may be explained by incomplete arterial transmission occurring in different regions at different times. Irrespective of aetiology, the pulsation may represent a failing microcirculation which indicates advanced venous disease.
The observation of pulsation in veins is not a novel one. Arterial-venous communications (fistulae) have been reported and proposed, and have even theorised to be a cause of varicose veins. Furthermore, phlebologists who perform perforating vein ablation associate venous pulsation as a marker of reduced success.
The identification of significant reflux (>0.5 seconds) has been given the lion’s share of attention as a cut-off point in clinical decision-making regarding haemodynamic suitability for treatment. Knowing that venous symptoms occur in healthy populations after standing for too long, and that significant reflux can occur in subjects without symptoms, a haemodynamic test that can define a cut-off point for clinical severity is eagerly awaited. Reflux tests abnormal reverse flow. The saphenous pulsation may emerge as a test for abnormal antegrade flow.
Work from our group (J Vasc Surg 2012; 56: 1338–43) compared saphenous pulsation in healthy volunteers with patients presenting for treatment. We observed that it was detectable in 75% of legs with great saphenous vein reflux and increased significantly with clinical severity and saphenous diameter. The presence of saphenous pulsation appeared to be a stronger marker of disease severity than the identification of reflux.
We acknowledge that our data on saphenous pulsation comes from a small series of subjects. However, given the ease at which it can be identified we recommend further research into this phenomenon. Avenues for its clinical potential include evaluations of significant haemodynamic disorder in epidemiological studies, its presence as a predictor of recurrent varicose veins prior to treatment and research into its exact aetiology in reconciling microcirculatory disturbances with haemodynamic disorder.
The recommendation is that the presence of saphenous pulsation should be reported in all duplex examinations of the leg veins. Its simplicity to record may provide us with an opportunity of defining a useful parameter of significant disordered flow in saphenous veins. Currently, this is not possible using reflux alone.
Christopher Lattimer and George Geroulakos are with Imperial College London, London, UK











