This article forms part of an educational supplement sponsored by Shockwave Medical. Explore the full Shockwave L6 series here.

Ashish Patel (Guy’s and St Thomas’ NHS Foundation Trust and King’s College London, London, UK) outlines a case report demonstrating how the new Shockwave L6 catheter represents a “significant addition” to clinicians’ armamentarium for the endovascular treatment of aortoiliac occlusive disease.
A 75-year-old female patient who was previously being treated for bilateral intermittent claudication with best medical therapy and ongoing watchful waiting was referred to our institution with rest pain in her right foot. She reported worsening of her symptoms bilaterally over the preceding six months. Her symptoms suggested short-distance claudication, with onset of pain in both of her calves after walking less than 25 metres. As a result of the new onset rest pain, she was not able to sleep, with her symptoms waking her up most nights during the course of a week. She was an ex-smoker, and her medical history included treated hypertension and hyperlipidaemia as well as stage 3A chronic kidney disease. She had previously undergone a left common femoral artery (CFA) to above-knee popliteal bypass using reversed great saphenous vein in 2008, which was confirmed to be patent on a recent Duplex scan with a moderate (20–49%) stenosis of the distal graft anastomosis. On clinical examination, she had cool feet bilaterally, with ischaemic rubor of her right toes. Her femoral pulses were weak bilaterally, and she had an ankle brachial pressure index (ABPI) of 0.4 on the left and 0.5 on the right.
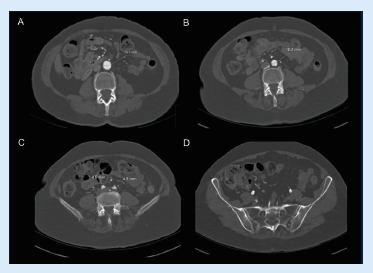
Computed tomography (CT) angiography revealed evidence of severe bilateral common iliac artery (CIA) stenoses from their origins, with diffuse heavy vascular calcification. She also had focal calcified stenoses of her external iliac arteries (EIAs) bilaterally and an occluded left internal iliac artery. During our multidisciplinary team discussion, it was noted that her distal aorta was very small (10.4mm) and more reasonably sized approximately 3cm above the bifurcation where it measured 14.7mm. In addition, her CIAs only measured 4.8–4.9mm on both sides (Figure 1). The technical options were discussed, including a covered endovascular reconstruction of the aortic bifurcation (CERAB) or high kissing stents into the larger segment of her aorta. However, given her previous left leg bypass, it was also noted that it was important to consider technical options that would preserve the aortic bifurcation to ensure she would have an ‘up and over’ access option, should the bypass (or her other outflow/run-off native vessels) require further endovascular intervention in the future. The planned recommended strategy was, therefore, to treat both CIAs and EIAs with intravascular lithotripsy (IVL) prior to covered stenting (with concomitant bare-metal stenting of the EIAs), in order to forego the need for either high kissing stents or a CERAB.
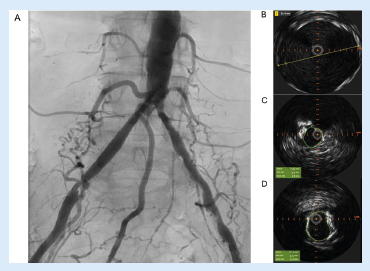
Due to her rest pain the procedure was performed under general anaesthesia. Bilateral CFA retrograde access was obtained, heparinisation commenced with target activated clotting time >200 seconds, and 7F sheaths advanced into both EIAs. Intravascular ultrasound (IVUS; Visions PV 0.014P, Philips) was used to accurately measure the distal aorta and both CIAs, which measured just 5.4mm and 4.1mm at their origins (Figure 2), but near 6–6.5mm distally. Intra-arterial digital subtraction angiography was used to confirm the bilateral CIA and EIA disease, accurately mark the aortic bifurcation and to carry out the remainder of the procedure using ‘image overlay’.
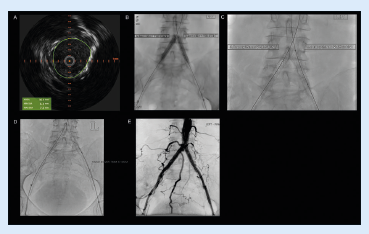
An 8mm Shockwave L6 IVL catheter was easily advanced into the right CIA and four cycles of IVL were delivered to this segment whilst supporting the contralateral CIA with a 6x40mm plain angioplasty ballon (Sterling balloon, Boston Scientific) that was inflated to nominal pressure (Figure 3). As a result of the need for minimal emitter overlap using the new Shockwave L6 device, we were able to treat a total of 5cm of diseased proximal iliac artery, with a further cycle of IVL delivered to the focal right EIA stenosis. In addition, we know that despite oversizing the Shockwave L6 catheter well beyond 50% for the proximal CIA, the semi-compliant balloon is never inflated above the lowest required pressure to achieve wall apposition, so the risk of vessel perforation is very low; this flexibility in sizing allows cost saving by enabling use of the same Shockwave catheter in the EIA segment. This process was repeated for the left CIA and EIA for the remaining five cycles. Repeat IVUS and angiography confirmed significant luminal gain in the treated segments (right CIA area increased from 17mm2 to 36mm2, Figure 4).
The procedure was completed by deploying an 8x39mm covered Gore Viabahn VBX stent graft (Gore Medial) very accurately into each CIA, below the aortic bifurcation (Figure 4). Below these, two bare-metal Zilver 635 self-expanding 7x40mm and 7x100mm stents (Cook Medical) were deployed to treat the right and left diseased EIA segments respectively, with IVUS used to mark distal healthy landing zones and to assess for adequate stent expansion. Final angiography showed brisk flow through the aortoiliac segments (Figure 4) with no evidence of distal embolisation and preservation of flow through the bypass graft and its run-off. A ProStyle (Abbott) was used for closure of the CFA access on both sides and check ultrasonography confirmed that both CFAs remained widely patent.
Duplex ultrasound follow-up at six weeks confirmed patency of all treated segments. The patient’s rest pain has fully resolved, she is no longer describing symptoms of claudication and has an ABPI of 0.9 bilaterally. This case demonstrates how IVL, when judiciously applied to the iliac segment, especially in cases of anatomical size mismatch between the aorta and iliac vessels, can be used to prevent the need for stenting into the aorta. The use of Shockwave L6 to lower the ‘stent zone’ by preparing the CIA origin also preserves future endovascular options by preserving the aortic bifurcation. In addition, the flexibility of the device with regards to sizing also allows for the treatment of calcium affecting the EIA in order to ensure maximum expansion of self-expanding stents deployed in this segment. In conclusion, the new Shockwave L6 IVL catheter is a significant addition to our armamentarium for the endovascular treatment of aortoiliac occlusive disease.
Ashish Patel is a consultant vascular and endovascular surgeon at Guy’s and St Thomas’ NHS Foundation Trust and a clinical senior lecturer in vascular surgery at King’s College London in London, UK. He is a paid consultant of Shockwave Medical and his views expressed are not necessarily those of Shockwave Medical.
Case images