This article forms part of an educational supplement sponsored by Shockwave Medical. Explore the full Shockwave E8 and Javelin series here.

The Shockwave Javelin peripheral intravascular lithotripsy (IVL) catheter “bridges a critical gap” in the management of chronic limb-threatening ischaemia (CLTI) in patients with complex multilevel disease. This is according to Ashish Patel and Narayanan Thulasidasan (London, UK), who here outline a case where the Shockwave Javelin offered a solution for “device-uncrossable” calcium.
Our early experience with the Shockwave Javelin peripheral IVL catheter suggests that, when applied in appropriately selected patients, it can provide a safe and reliable means of bridging the gap between wire crossing and vessel preparation, restoring straight-line flow to the foot and broadening treatment options for patients with multilevel disease and advanced tissue loss.
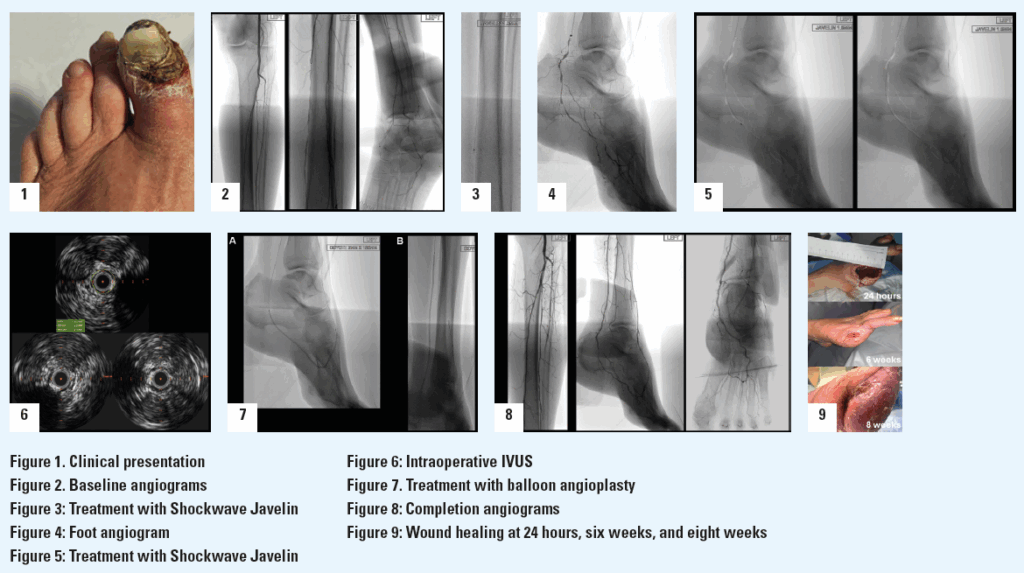
A 71-year-old woman was referred with a three-month history of progressive discolouration of the left hallux, which had become globally dusky with dry gangrene affecting the distal phalanx (Rutherford Category 5; Figure 1). She also had severe nocturnal rest pain that had been disrupting her sleep for several months. She continued to smoke and had a history of hypertension and hyperlipidaemia, but no other significant comorbidities. Examination revealed the left foot to be cooler than the right, with a weak popliteal pulse and absent pedal pulses. Doppler assessment demonstrated monophasic dorsalis pedis and posterior tibial signals, with an ankle–brachial pressure index (ABPI) of 0.3. Arterial duplex ultrasonography showed significant stenotic disease within the mid-segment of the superficial femoral artery (SFA) and multilevel tibial disease involving both her posterior and anterior tibial arteries. During our multidisciplinary team (MDT) discussion, it was noted that both her posterior tibial and lateral plantar arteries contained multiple focal calcific steno-occlusive lesions. The extent and distribution of this calcification was anticipated to present a considerable technical challenge, particularly in tracking catheters or advancing angioplasty balloons into the target vessels beyond these lesions. After reviewing the imaging and clinical context, the consensus opinion of the MDT was that an endovascular-first approach would be the most appropriate treatment strategy, proceeding to amputation of the left hallux during the same procedure if the planned recanalisation was successful. It was also agreed that to maximise the chance of durable healing post-amputation, revascularisation should establish direct ‘straight-line’ flow into the foot, with specific attention to reconstituting the lateral plantar artery and the plantar arch.
Given the severity of her rest pain and the anticipated technical challenges, the procedure was carried out under general anaesthesia for both patient comfort and procedural control. Under ultrasound guidance, antegrade left common femoral artery (CFA) access was obtained using a micropuncture kit and a 6Fr sheath then advanced into the proximal SFA. Heparinisation was commenced with a target activated clotting time >200 seconds. Intra-arterial digital subtraction angiography confirmed the duplex findings, with mid-SFA lesions in addition to multilevel occlusive lesions in both the posterior tibial and anterior tibial arteries (Figure 2). Angiographic runs of the foot revealed a heavily diseased lateral plantar artery (the main target vessel in the foot for this case) and an incomplete foot arch (Figure 2). Intravascular ultrasound (IVUS; Visions PV .014P RX, Philips) was used to accurately define the extent and morphology of the SFA lesions, as well as to obtain precise vessel diameter measurements. The SFA was then treated with 5mm plain balloon angioplasty (Sterling, Boston Scientific), followed by a 5x200mm drug-coated balloon (Ranger, Boston Scientific). Attention was then turned to the posterior tibial artery, which was crossed using an 0.014” Asahi Gladius MG ES wire (Asahi Intecc) supported by an angled 0.014” support catheter (CXI, Cook Medical). Given the difficulty in tracking the CXI through the distal posterior tibial vessels and the presence of the focal lateral plantar artery lesions seen on angiography, we decided that the Shockwave Javelin would be ideally suited for calcium modification in this scenario.
The Shockwave Javelin tracked without difficulty to the mid-posterior tibial artery, where three treatment cycles (30 pulses in total) were delivered to the mid and distal segments (Figure 3). This calcium modification allowed the catheter to easily pass into the ankle. At this point, a selective angiogram of the pedal arch was performed through the Shockwave Javelin catheter to delineate the anatomy of the foot vasculature in greater detail (Figure 4). Using a combination of 0.014” Asahi Halberd and Gladius MG ES wires, the lateral plantar artery and plantar arch were successfully crossed. Seven further cycles of the Shockwave Javelin (70 pulses) were used to treat the lateral plantar artery, plantar arch and the dorsalis pedis artery (Figure 5). Following this, both the IVUS catheter (Figure 6) and a low-profile 0.014” balloon (Coyote, Boston Scientific) could now be advanced without resistance into the foot vessels, reflecting the marked improvement in vessel compliance after successful calcium modification with the Shockwave Javelin. The plantar arch and lateral plantar artery were treated with a 2x150mm angioplasty balloon (Figure 7A). Following sizing with IVUS, the posterior tibial artery was treated (Figure 7B) with a 2.5x220mm balloon (Coyote, Boston Scientific). Notably, in the distal posterior tibial artery and plantar vessels, balloons expanded to their nominal diameter at just 6atm, highlighting the significant compliance gain post-IVL. The anterior tibial artery was then crossed and treated using the same balloon at 12atm.
Completion angiography demonstrated significant luminal gain in the posterior tibial, lateral plantar, plantar arch and dorsalis pedis vessels, with brisk preferential flow into the posterior tibial and lateral plantar vessels and a widely patent pedal arch (Figure 8). There was some vasospasm in the proximal anterior tibial artery. IVUS also confirmed good luminal gain and the restoration of visible pulsatility within the lateral plantar artery, which had not been present prior to treatment with the Shockwave Javelin.
A closure device (MynxControl, Cordis) was used for closure of the CFA access and check ultrasonography confirmed that the CFA remained widely patent. The patient then underwent ray amputation of her left hallux during the same procedure, where it was noted that there was pulsatile bleeding of the wound bed. The amputation site was left open to heal by secondary intention (Figure 9) and she had an uneventful postoperative recovery. The patient was reviewed regularly in our dedicated vascular foot clinic following discharge, with dressing changes performed by community nursing teams under close communication with our service. At her two-week follow-up, the amputation site was healthy, with evidence of granulation tissue and no signs of infection. She also reported complete resolution of her rest pain. At eight weeks, the amputation site had fully healed (Figure 9) and the patient’s ABPI had improved from a preoperative value of 0.3 to 0.8. She had resumed independent ambulation and was engaging with smoking cessation services.
This case illustrates the unique capability of the Shockwave Javelin to address one of the most persistent technical barriers in complex tibial and pedal revascularisation—the ‘device-uncrossable’ calcified lesion. In this patient, both the posterior tibial and lateral plantar arteries contained multifocal heavily calcified steno-occlusive disease that was expected to prevent the passage of even low-profile angioplasty balloons. The successful outcome underscores the unique value of the Shockwave Javelin in CLTI, particularly in the setting of diffuse, heavily calcified tibial and below-the-ankle (BTA) disease. By safely and predictably modifying calcific plaque, the Shockwave Javelin enables delivery of definitive therapies, such as balloon angioplasty, to distal target vessels that are often otherwise inaccessible, restoring straight-line flow to the foot and re-establishing an intact pedal arch. In this case, achieving luminal gain in the lateral plantar artery and plantar arch was essential for wound healing following hallux amputation and would have been extremely challenging without calcium modification.
A key procedural finding was the marked improvement in vessel compliance following IVL, demonstrated by low-pressure balloon expansion to nominal diameter in the distal tibial and pedal arteries and the absence of recoil on IVUS. These changes were achieved without flow-limiting dissection, perforation, or distal embolisation, complications that remain a concern during vessel preparation in this territory. As an enabling technology for effective endovascular treatment of tibial and BTA vessels (territories where few reliable options have previously existed) the Shockwave Javelin bridges a critical gap in the management of CLTI in patients with complex multilevel disease.
Case images
 Ashish Patel is a consultant vascular and endovascular surgeon at Guy’s and St Thomas’ NHS Foundation Trust and a reader in vascular surgery and sciences at King’s College London in London, UK. He is a paid Shockwave Medical consultant.
Ashish Patel is a consultant vascular and endovascular surgeon at Guy’s and St Thomas’ NHS Foundation Trust and a reader in vascular surgery and sciences at King’s College London in London, UK. He is a paid Shockwave Medical consultant.
Narayanan Thulasidasan is a consultant interventional radiologist at Guy’s and St Thomas’ NHS Foundation Trust and a paid Shockwave Medical consultant.
The views expressed in this article are those of the physicians and may not reflect the views of Shockwave Medical.










