This article forms part of an educational supplement sponsored by Shockwave Medical. Explore the full Shockwave L6 series here.

Mark Portou (Royal Free Hospital, London, UK) presents the case of a patient with chronic limb-threatening ischaemia (CLTI) in whom use of the new Shockwave L6 resulted in avoiding the need for a stent, thereby reducing risk to the patient and preserving future access options.
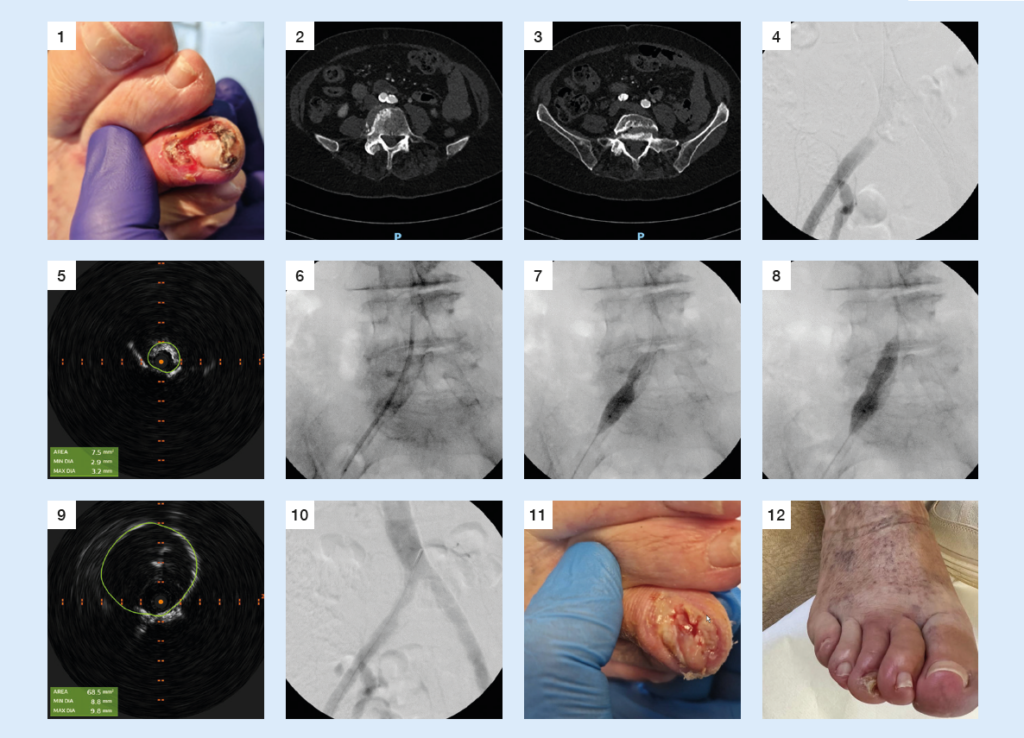
An 86-year-old woman with a longstanding history of right-sided, exercise-induced buttock and thigh pain presented acutely to our clinic with a deteriorating right third toe wound and infection following an injury. At initial presentation, she had an absent right femoral pulse, and a cyanotic right third toe with ulceration and evidence of a soft tissue infection (Figure 1). The patient had a background of bilateral total hip replacements, diabetes mellitus, hypertension and ischaemic heart disease with compensated heart failure.
A computed tomography (CT) angiogram revealed a calcified aortic bifurcation (Figure 2) and a focal near-occlusive calcified plaque in the proximal right common iliac artery (CIA; Figure 3). Following urgent outpatient review, she was placed on the next operating list. Her treatment options included open surgical bypass with a very high perioperative risk or, more likely, an endovascular approach. Before the availability of calciummodification technologies, optimum endovascular treatment would have inevitably required the insertion of at least one stent. The risk of a stent-only approach in this situation given the very tight stenosis would have been under-expansion of the stent and risk of subsequent symptom recurrence or stent thrombosis. Likewise, the insertion of a covered stent risked the patent internal iliac, and the possibility of kissing stents, limiting access options for future interventions.
A retrograde right percutaneous common femoral artery puncture was made under ultrasound guidance using a micropuncture sheath. The iliac lesion was crossed into the aorta and an 8F Brite Tip sheath (Cordis) was placed over an Amplatz wire. Both retrograde and antegrade digital subtraction angiography confirmed a near-occlusive stenosis of the right CIA (Figure 4). A low-contrast angiography approach was used to illustrate flow, augmented with a 0.018” intravascular ultrasound (IVUS) catheter to measure reference vessel diameter (RVD), confirm luminal position, and delineate lesion location, length, composition, and severity of stenosis. A RVD of 10.2mm was measured. The mean luminal area of the pre-occlusive stenosis was measured to be 7.5mm2 (Figure 5). A 3mm pre-dilation with a 3x100mm Sterling balloon (Boston Scientific) over an 0.018” V18 guidewire (Boston Scientific) was performed (Figure 6).
For this case, we chose to use the new Shockwave L6, which provides optimal sizing in the iliac arteries. The catheter was passed across the lesion, and inflated to 2 then 4atm. The low inflation pressures provide safe oversized expansion in high-risk vasculature. The device was placed across the focal calcific lesion, repositioned across it, and a total of 300 pulses were delivered (Figures 7 and 8). From Figures 7 and 8 you can see, as more energy is delivered to the artery, the vascular compliance of the vessel changes, and the integrated balloon in the Shockwave L6 catheter begins to increase in size. Post intravascular lithotripsy (IVL), IVUS demonstrated significant lumen gain, with an increase in minimal lumen area (MLA) to 68.5mm2, and no evidence of dissection (Figure 9). Following the use of the Shockwave L6 catheter, we had achieved excellent luminal expansion. IVUS and further angiography were performed to assess for vessel recoil and extent of lumen gain. There was sufficient lumen gain and no flowlimiting dissections; therefore, we elected for no further balloon dilatation, and no stent was deployed.
The post-procedure IVUS and final antegrade digital subtraction angiography images confirmed a residual stenosis less than 30%, with a 30% or less post-treatment residual stenosis providing a longer-term marker of procedural success (Figure 10). Haemostasis was achieved with an 8F Angioseal (Terumo Interventional Systems), with an immediate return of the right femoral pulse noted. One week post procedure the patient reported complete resolution of pain and a significant improvement in the third toe wound (Figure 11). They were completely healed by six weeks (Figure 12) and are now walking unlimited distances pain free.
Prior to the availability of Shockwave L6, this lesion would have required placement of a stent, possibly kissing stents. As mentioned earlier in this report, this would have led to certain challenges for this patient by limiting access options as the likelihood of a patient with CLTI requiring further treatment in the future is high. In our practice, patients require surveillance arterial Duplex scans at regular intervals post stent insertion.
Patients with CLTI must be considered in the same manner as cancer patients, with a progressive disease that, post treatment, at best, should be considered as entering a state of remission. Preserving future access options is key to the long-term management of these patients. The Shockwave L6 IVL catheter now brings the safe and effective IVL technology to the larger diameter vessels. The low-pressure inflation technique and ability to increase vessel wall compliance through medial wall and intimal plaque calcium modification present a genuine opportunity to change the paradigm for calcified iliac and common femoral disease. In the situations where stents are required, adequate vessel preparation will result in better stent expansion and reduce the need to stent above the bifurcation into the aorta. This case demonstrates, however, that lumen gain can be achieved through the actions of IVL alone, without the need for balloon post dilatation or stent insertion, reducing risk and preserving options.
Mark Portou is a consultant vascular surgeon at the Royal Free Hospital in London, UK. He is a paid consultant of Shockwave Medical and his views expressed are not necessarily those of Shockwave Medical.
Case images