Virtual models can be created in the angiography room thanks to an approach developed by researchers at the University of Montreal Hospital Research Centre (CRCHUM), Canada, and the university’s departments of radiology, radiation oncology, and nuclear medicine. The latest advances were presented by Gilles Soulez at the Cardiovascular and Interventional Radiology Society of Europe (CIRSE) conference (26–30 September, Lisbon, Portugal).
Soulez has been involved in developing medical imaging technologies to prevent complication for, operate on, and monitor patients with abdominal aortic aneurysms (AAA) for 25 years. The main problem he has faced has been the ability to properly visualise the area to be treated. “Remarkable advances in imagery have improved surgery and helped to develop less invasive interventions. But the images are still far from being perfect. We want to develop new software to maximise the use of images generated with current ultrasound, scanning, and magnetic resonance imaging (MRI) technologies to ultimately provide more personalised treatments,” he explained.
Currently, an abdominal ultrasound or measurement of the aorta with a scanner can detect patients at risk of aneurysm rupture. Beyond 5cm for women and 5.5cm for men, surgery is usually recommended. However, operations carry their own risks, so researchers want to refine screening to provide the most appropriate treatments for patients who really need surgery.
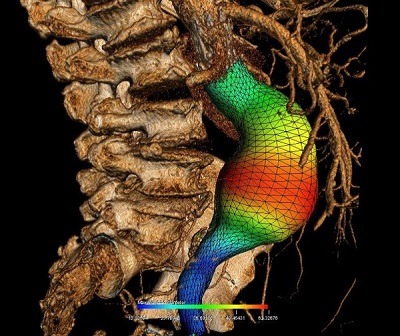
To avoid rupturing an AAA, two treatment options exist—open surgery to replace the diseased section or endovascular grafting. The latter option is less invasive, but in some patients, the morphology of the aneurysm is not suited to this kind of treatment. Using scanner images, Soulez’s research provides 3D images of all components of the aneurysm—the light, the thrombus or clot, the wall, and the calcification. “The grid is used to establish growth profiles of the aneurysm. We are now working to create simulations to better predict the risk of rupture, adding biomechanical properties such as tissue elasticity and connectivity at each pixel of the grid,” he explained.
Simulations will also help in the operating room. Currently, the operation is performed using static images taken by a scanner before the procedure. The procedure itself is done under fluoroscopy by injecting dye into the vessels to be treated. “The image produced by X-ray shows the dye in the vessels and the stent being inserted, but not the wall. This approach requires a lot of dye, which can be toxic for the patient if used in excessive amounts,” said the radiologist.
Thanks to a grant from the Canadian Institutes of Health Research (CIHR), in partnership with Siemens, Soulez’s laboratory has been able to develop this approach that combines all available data. “We superimpose the images, and this helps to visualise the area to be treated. But in reality, the tools we introduce into the body during the procedure deform the organs. We are testing at the CHUM and in Halifax right now a new approach that uses a computer to automatically recognise the tools introduced into the body and correct the deformities they cause,” he said. “We hope this simulation-operation model will improve the accuracy of the procedure.”
Soulez’s research in interventional radiology also aims to ensure that the devices installed in patients fit in place and avoid aneurysm rupture. Following the stent-graft operation, patients undergo annual scans. A new ultrasound technology called elastography that was developed in collaboration with Guy Cloutier, also of the University of Montreal Hospital Research Centre, holds the promise of not only effectively identifying leaks, but also evaluating how the aneurysm is healing. Another option is the bioactive stent and injection of a gel around the implant in order to prevent or stop leaks. These new biomaterials are being developed in collaboration with Soulez and Cloutier’s colleague Sophie Lerouge.











