
Michele Piazza (Padua, Italy) advises how to manage the challenging anatomical scenario of a narrow aorta during fenestrated and branched endovascular aneurysm repair (F/BEVAR), highlighting accurate, patient-specific planning and use of the correct bridging stent technology as the keys to good results.
Endovascular treatment of complex abdominal aortic aneurysms (AAAs) and thoracoabdominal aortic aneurysm (TAAAs) with fenestrated and branched endografts, or F/BEVAR, today represents a valid alternative to open repair, thanks to its association with lower morbidity and mortality. Generally, these aneurysms are characterised by extensive involvement of the aorta, with visceral segment management being the real challenge. Some anatomical features such as a narrow or angulated aorta increase the complexities of repair, not only in terms of technical feasibility, but also in terms of target vessel complications and material resistance to fatigue.
The main issue with a narrow paravisceral aorta relates to the lack of space, which may lead to inadequate expansion of the main aortic endograft, as well as conflicts between or compression of the bridging stents. Also, aortic angulation is one of the major causes of target vessel instability, primarily in relation to kinking, and its association with a narrow paravisceral aorta may worsen outcomes exponentially.
To date, the only parameter that has defined a narrow paravisceral aorta is a transverse maximum diameter of ≤25mm, while a risky aortic angle is >45°. However, other concomitant anatomical aspects may play a role in defining outcomes, including wall quality, narrowing extension, and the type of endograft and bridging stents used. We recently published our results demonstrating that in FEVAR, a narrow paravisceral aorta of <20mm in association with a >30° aortic angle or no vertical distance between the renal arteries was a predictor of target vessel instability and particularly that which causes occlusion.
This is probably because a narrow paravisceral aorta can often create conflicts between the multiple flared segments of two (renal) or three (two renal and the superior mesenteric artery [SMA]) bridging stents protruding at the same level within the main aortic fenestrated endograft. This geometrical structure exposes the procedure to the risk of lower technical success and worsens short-term outcomes, caused by inadequate flaring of one or more bridging stents, or stent compression or collapse during other concomitant endovascular manoeuvres, such as the deployment of a distal bifurcated device.
Today, several custom-made device conformations are available for elective complex AAA cases, and the possibility of switching a plan from a four-fenestrated graft to a combination of fenestration and inner branches may help to overcome this complex anatomic dilemma. A case example is depicted in Figure 1. In the case of a complex AAA with a narrow pararenal aorta and an SMA and renal arteries originating at the same level, the use of two fenestrations for the coeliac trunk and SMA and two inner branches for the renal arteries allow for the spatial differentiation of the inlet of the three vessels. The SMA will have a single flared bridging stent, protruding perpendicularly from the anterior wall of the main graft as usual, while the two renal arteries will have their inlet 2cm above, at a 90° clockwise position, thus avoiding cumbersome protrusion conflicts.
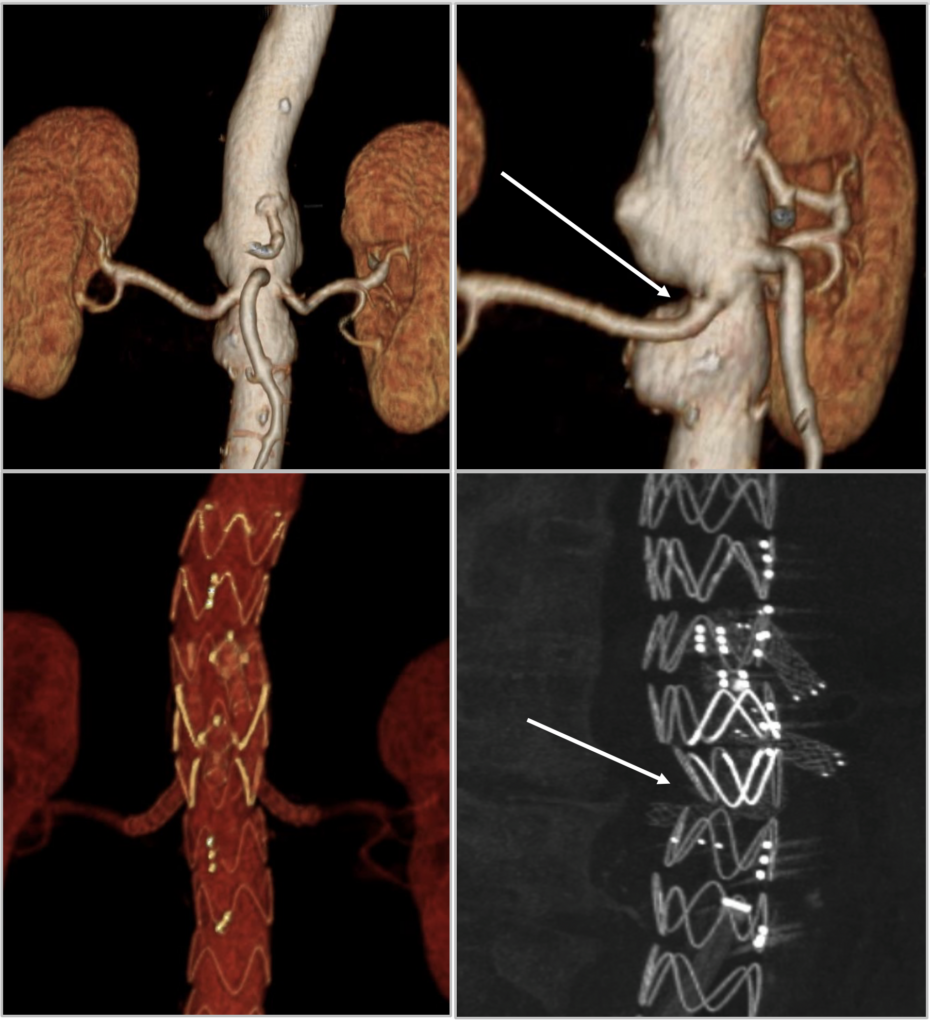
As previously reported by other expert centres, a potential issue in using inner branches for the renal arteries may be the higher risk of instability. For this reason, it is mandatory to use patient-specific, custom-made devices with dedicated planning, with the ostium of the renal arteries positioned in the lowest part of the diamond, to favour a smooth bridging stent transition. Also, it is of paramount importance to optimise the choice of bridging stents, using either self-expanding, balloon-expandable, or a combination of both, depending on the specific anatomical course.
In this conformation, the use of inner branches for the renal arteries also allows for a short covering length above the coeliac trunk, compared to the longer coverage that would be required to allocate outer branches, thus exposing the patient to a lower risk of spinal cord ischaemia.
Other potential planning options, as well as new technological characteristics, are emerging in the market. For example, the ‘semibranch’, which is an intermediate solution between a fenestration and a branch, has possible applications in cases involving narrow and angulated aortas.
In extent type II and III TAAAs, which generally carry a large aneurysmal sac, planning may include several possible custom-made device conformations using fenestrations, outer branches or inner branches. To be clear, outer branches have been demonstrated to work in both large and narrow aortas with good outcomes. In particular, the use of off-the-shelf inner or outer branches is feasible with any aortic diameter, even if a theoretical landmark is historically set for outer branches at 25mm.
In our study, a narrow paravisceral aorta by itself was not a problem for outer branches; the only condition that increased the risk for occlusion was the presence of a long-segment longitudinal extension of the narrow aorta or a narrow aorta with circumferential wall calcifications. This is clearly because there is a fixed narrow space with no adaptability for complete outer-branch expansion or multiple-branch course. When planning, do not focus on the narrowness; instead, consider the quality of the wall in the narrow region. Frequently, the narrow inner lumen represents a virtual space, with the surrounding area occupied by soft thrombus material. In terms of technology, preloaded branches may have a role; these may help in a narrow area to make catheters progress with more support.
Using a main graft with nitinol stents in the narrow area may increase conformability and be able to surround the space where branches lie rather that compressing them.
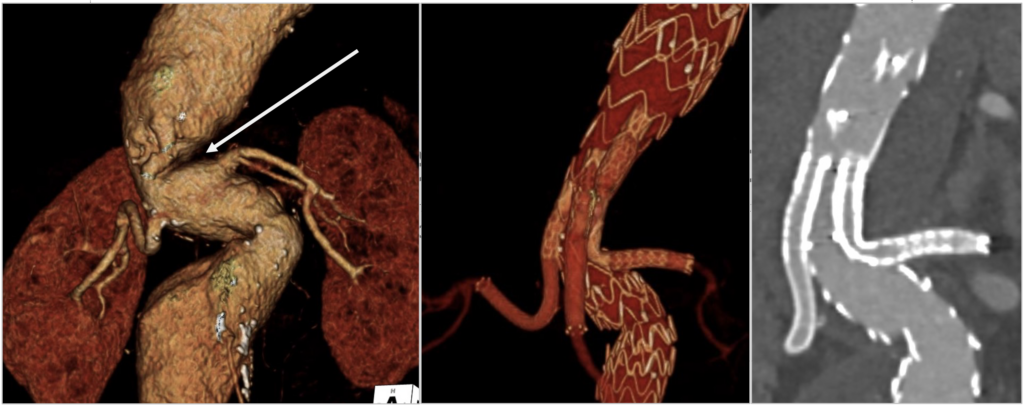
What about the right bridging stent? Plan which one to use, rather than working with what you have in stock that day. Self-expanding stents guarantee adequate distal adaptability and transition to target vessel, as well as smooth conformation in cases involving tortuosity or angulation. On the other hand, balloon-expandable stents may allow for the maintenance of an adequate diameter in a severely angulated narrow aortic region, thanks to their strong radial force, and sometimes the combination of both may be useful for success (Figure 2). So, please anticipate how your main graft, branches, and fenestration will conform to the narrow anatomy and plan accordingly.
What about a narrow paravisceral true lumen in post-type B aneurysms? More studies are yet to come. Is it a real narrow? Or is it a virtual space? Again, new technologies such as endoseptotomy are helping us to erase the narrow lumen and create a single, large-space true–false for correct main graft deployment and accommodation.
Today, FEVAR and BEVAR are both feasible in a narrow paravisceral aorta and overall provide satisfactory results. In this complex anatomic scenario, accurate patient-specific planning with both custom-made devices and off-the-shelf conformations—as well as use of the correct bridging stent technology—are mandatory to ensure a higher rate of success and long-term durability.
Michele Piazza is a professor in vascular surgery at the University of Padua (Padua, Italy). He is a consultant for Cook, Artivion and WL Gore, with all fees paid to the Department of Cardiac, Thoracic, Vascular Science and Public Health at the University of Padua.











