This article forms part of an educational supplement sponsored by Shockwave Medical. Explore the full Compliance is Key series here.

Giacomo Isernia and Gioele Simonte (Azienda Ospedaliera di Perugia, Perugia, Italy) outline a branched endovascular aneurysm repair (BEVAR) case in which the M5+ Intravascular Lithotripsy (IVL) catheter (Shockwave Medical) was “effective in modifying arterial compliance to provide luminal gain and reduce procedural complications”.
The Perugia vascular and endovascular team has been a strong believer in the endovascular revolution since the early nineties, exploring the possibilities provided by new devices to treat aortic and thoracic disease.
Nowadays, iliofemoral accesses represent one of the most important concerns when dealing with complex aortic repair. Many custom-made or off-the-shelf thoracoabdominal endografts require large-bore sheaths to facilitate delivery, and for patients with diseased, calcified vascular accesses this can lead to complications with both perioperative and long-term morbidity and mortality,1 which forces physicians to modify their approach and prevents perfect tailoring to the vascular anatomy.

Shockwave IVL (Shockwave Medical) expands feasibility and safety during these challenging procedures, allowing a complete endovascular management by delivering sonic pressure waves into the vessel wall to fracture superficial and deep calcium. This changes vessel compliance, creating more elasticity in the vessel and thus granting the possibility to take into account only visceral vessels and aortic features, overcoming most of the vascular accesses’ limitations.
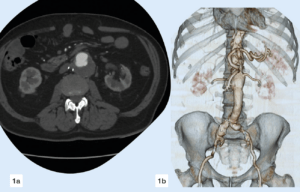
Herein we report the case of a 75-year-old male patient treated in 2009 for infrarenal ruptured abdominal aortic aneurysm (AAA) who developed a proximal pararenal anastomotic pseudoaneurysm of 55mm in maximum axial diameter (Figure 1).
As the patient was a poor candidate for open repair, we opted for an E-nside four-inner-branched, pre-cannulated endograft (Artivion). The major concern about the proposed approach was that the vascular accesses as a tight circumferential calcified stenosis affected the bilateral origins of the common iliac arteries (Figure 2). Because of this obstructive disease, the femoral pulses were weak, with biphasic wave form bilaterally detected by duplex ultrasound during preoperative evaluation.
Furthermore, two large lumbar arteries arose from the aortic bifurcation and therefore the plan consisted of a distal landing inside the previous aorto-aortic surgical graft, avoiding sacrificing these vessels in order to reduce the risk for spinal cord ischaemia (Figure 3). Moreover, the aortic arch and descending thoracic aorta, as shown in Figure 4, presented irregular floating thrombotic apposition, imposing the need to avoid an upper extremity access and thus the need for both iliac arteries to accomplish endovascular reconstruction.
After preparing both femoral accesses for percutaneous manipulation with two Proglide vascular closure devices (Abbott) using the pre-close technique, an M5+ 8x60mm catheter was advanced over a 0.014” just at the level of the right common iliac artery stenosis, delivering five cycles of energy (150 pulses overall; Figure 5). The new M5+ catheter halves the time needed for treatment, doubling the pulse delivery to two pulses per second. The exact same procedure was repeated using the remaining five cycles of energy with the same catheter on the contralateral side, to further modify the vessel compliance at the origin of the left common iliac artery.
After vessels preparation, a 24Fr Dryseal introducer sheath (W L Gore) was easily advanced from the right percutaneous common femoral access until reaching the surgical infrarenal aortic graft lumen. The E-nside off-the-shelf endograft was finally deployed through the Dryseal sheath at the planned position.
Taking advantage of the left common femoral access, a 16Fr introducer sheath (Cook Medical) was smoothly inserted until the distal edge of the just-released inner-branched endograft. An additional steerable 12Fr Reach introducer sheath (Oscor) was coaxially pushed and bent at the cranial edge of the endograft.
In this favourable configuration, exploiting both femoral accesses and the inner branched pre-cannulated technology, visceral artery bridging was effortlessly and promptly completed.
Control angiography was performed using a CO2 automatic injector (Angiodroid) because of a moderate renal impairment. The resulting angiography showed effective pseudoaneurysm exclusion with patent target visceral vessels without signs related to possible iliac complications (i.e. dissection, rupture, thrombus).
In summary, Shockwave IVL was effective in modifying arterial compliance to provide luminal gain and reduce procedural complications. Postoperative duplex assessment revealed a polyphasic wave in both common femoral arteries as well as a clinically noticeable pulse improvement.
A control computed tomography angiography (CTA) was performed on postoperative day two as per institutional protocol, confirming the intraoperative findings and revealing a significant luminal gain at the treated segments that was especially evident on the right (Figure 6).
Case images





References
- O Donnell TFX, Deery SE, Boitano LT, et al. The long-term implications of access complications during endovascular aneurysm repair. J Vasc. Surg. 2021 April;73(4):1253–1260.
Giacomo Isernia is a vascular surgeon at the Azienda Ospedaliera di Perugia in Perugia, Italy.
Gioele Simonte is a vascular surgery consultant at the Azienda Ospedaliera di Perugia.











