This article forms part of an educational supplement sponsored by Shockwave Medical. Explore the full Compliance is Key series here.

In this case report, Narayanan Thulasidasan (Guy’s & St Thomas’ NHS Foundation Trust, London, UK) demonstrates how the M5+ Intravascular Lithotripsy (IVL) catheter (Shockwave Medical) has transformed endovascular treatment options for the common femoral artery (CFA), “opening up minimally invasive therapy to many more patients considered high risk for open surgery without compromising on effectiveness”.
Endovascular treatment of the CFA was first indirectly reported in 19941 and then specifically in 2004.2–3 However, two decades later—despite multiple single-arm studies, a small RCT,4 and a recent retrospective propensity-matched comparison of over a thousand cases5—it remains at best infrequently utilised outside a small number of centres, and at worst regarded with outright hostility. At our institution we take a pragmatic approach; whilst the majority of patients with symptomatic CFA atherosclerotic disease continue to be treated with common femoral endarterectomy and patch plasty, we do consider endovascular treatment of the CFA in patients with elevated perioperative risk (of wound infection or from an anaesthetic perspective), and those with high frailty score/poor mobility and/or shorter life expectancy.
In chronic limb-threatening ischaemia (CLTI) patients for whom endovascular treatment of the CFA is deemed most appropriate, careful consideration must be given to the choice of technique. Distribution of disease (including involvement of the profunda femoris artery [PFA] origin), CFA diameter, and, importantly, the presence of nodular calcification—which frequently occurs in CFA lesions and predicted poorer outcomes in the CAULIFLOWER study5— must all be taken into account. Due to the suboptimal response of such heavily calcified lesions to simple balloon angioplasty without prior vessel preparation, these patients were often previously excluded from endovascular treatment of the CFA if they had arteries that were too large for Supera (Abbott) stenting, or patency of both the PFA and superficial femoral artery (SFA), conferring increased risk of distal embolisation from atherectomy. IVL, however, with its exceptional safety profile (0% distal embolisation and 0.7% type D–F dissection)6 and our own experience of its strong performance in this lesion type, has shifted the paradigm for risk and efficacy of treatment of the CFA in this setting.
An 89-year-old female patient was referred to our institution with bilateral painful legs and a large, deep, infected pre-tibial ulcer on the right. Her medical history included hypertension, hyperlipidaemia, chronic obstructive pulmonary disease, chronic kidney disease (stage 3a), osteoarthritis and restless leg syndrome, and she was noted to have iron-deficiency anaemia and new atrial fibrillation. Computed tomography angiography (CTA) at the referring hospital revealed diffuse heavy vascular calcification, patent right iliac arteries, multifocal stenotic disease in the CFA and SFA and then a heavily calcified chronic total occlusion (CTO) of the popliteal artery reconstituting in the P3 segment with three-vessel tibial run-off.
The possibility of primary below-knee amputation was discussed, but the patient was understandably adamant that she did not want this, as her mobility was already restricted and she feared losing what independence she had left. Therefore, with the primary objectives of limb salvage and pain control, a multidisciplinary team decision was made to attempt total endovascular revascularisation. Due to continuous lower limb movement secondary to restless legs syndrome, the procedure was performed under general anaesthesia (using a totally intravenous technique to reduce the risk of postoperative delirium). The planned strategy was to treat the right CFA with IVL from a contralateral groin approach, thus facilitating antegrade right CFA access, which would expedite crossing and primary stenting of the popliteal CTO in order to minimise the anaesthetic time in this multi-morbid patient.
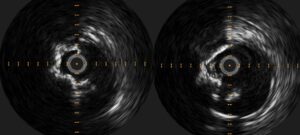
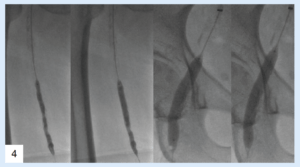
Left CFA retrograde access was obtained, heparinisation commenced with target activated clotting time >200 seconds, and a 7Fr crossover sheath (Flexor Balkin, Cook Medical) advanced to the right external iliac artery (EIA). Intravascular ultrasound (IVUS; EagleEye, Philips) was employed in order to minimise use of iodinated contrast, revealing 60% right CFA stenosis with reference vessel diameter between 8 and 9mm. An 8mm M5+ catheter was easily advanced to the 5.5mm-diameter right SFA, and five cycles of IVL were delivered to its stenotic proximal/mid segments. With experience, we are comfortable oversizing the Shockwave catheter well beyond the minimum recommended 1.1:1 ratio, as the semi-compliant balloon is never inflated above the lowest required pressure to achieve wall apposition so the risk of dissection is extremely low. This flexibility in sizing allows significant cost saving by enabling use of a single Shockwave catheter at multiple levels. The M5+ catheter was then withdrawn to the right CFA and a further five cycles of IVL delivered, with slight adjustments in the position of the catheter between cycles to vary the incident angle of the lithotripsy pulse on the calcium. After IVL vessel preparation, plain balloon angioplasty (Sterling, Boston Scientific) was performed to 5mm in the SFA and 8mm in the CFA, followed by application of a 6mm paclitaxel-coated balloon (Ranger, Boston Scientific) to the SFA. Repeat IVUS and angiography confirmed significant luminal gain in the treated segments, and, importantly, no dissections in the right CFA.
Using a micropuncture technique, ultrasound-guided antegrade access to the right CFA was then obtained in the segment treated with IVL, and a 6Fr sheath easily inserted. For speed, subintimal crossing of the popliteal CTO with a Hi-Torque Command 18 ST guidewire (Abbott) was accepted, with targeted re-entry to the proximal P3 segment using an Outback catheter (Cordis). The CTO was pre-dilated to high pressure with a 6mm Athletis balloon (Boston Scientific), facilitating nominal deployment of a 5.5x200mm Supera stent from P3 to the distal SFA. IVUS demonstrated the proximal end of the stent had landed in a residual stenosis, so proximal extension with a 6mm BioMimics3D stent (Veryan Medical) was undertaken. Completion IVUS and angiography confirmed excellent stent position, expansion and flow with preservation of the three-vessel run-off. A ProStyle (Abbott) was used for closure of the 7Fr left CFA access, and manual compression for the 6Fr right CFA access. Check ultrasonography confirmed the right CFA remained widely patent.
Ultrasound follow-up at five months confirmed patency of all treated segments, and the patient has experienced a significant reduction in pain (which is now confined to the location of the slowly healing ulcer) and retains her mobility. This case demonstrates how IVL applied to the CFA not only effectively treats calcified plaque, but can also enable immediate percutaneous access to optimally treat more distal disease by changing the vessel compliance sufficiently to facilitate antegrade puncture. We consider IVL to be a significant addition to our armamentarium for the endovascular treatment of the CFA, opening minimally invasive therapy to many more patients considered high risk for open surgery without compromising on effectiveness.
Case images




References
- Mandalam KR, Rao VR, Sandhyamani S, et al. Focal occlusive disease of the common femoral artery: a report of 20 cases. Cardiovasc Surg. 1994 Aug;2(4):498–502.
- Silva JA, White CJ, Quintana H, et al. Percutaneous revascularization of the common femoral artery for limb ischemia. Catheter Cardiovasc Interv. 2004 Jun;62(2):230–3.
- Stricker H, Jacomella V. Stent-assisted angioplasty at the level of the common femoral artery bifurcation: midterm outcomes. J Endovasc Ther. 2004 Jun;11(3):281–6.
- Gouëffic Y, Della Schiava N, Thaveau F, et al. Stenting or surgery for de novo common femoral artery stenosis. J Am Coll Cardiol Intv. 2017 Jul;10 (13):1344–1354.
- Nakama T, Takahara M, Iwata Y, et al. One-year outcomes of thromboendarterectomy vs endovascular therapy for common femoral artery lesions: CAULIFLOWER study results. JACC Cardiovasc Interv. 2022 Jul 25;15(14):1453–1463.
- Armstrong EJ. Intravascular Lithotripsy for the treatment of peripheral artery calcification: results from the Disrupt PAD III observational study. Oral presentation at VIVA 2022, late-breaking clinical trials session.
Narayanan Thulasidasan is a consultant interventional radiologist at Guy’s & St Thomas’ NHS Foundation Trust in London, UK.












Love your work Dr Narayanan! As a former patient of yours, it’s always interesting to see your work,(even if I don’t understand a word of the medical lingo). Keep rocking !
Ross 🙂