Remote ischaemic conditioning is a “really innovative technology” that can be used as an adjunctive therapy to significantly reduce tissue damage from an interrupted blood supply, Matthew Regulski (medical director, The Wound Institute of Ocean County New Jersey; partner, Ocean County Foot and Ankle Surgical Associates, Manahawkin, USA) enthused during the Symposium on Advanced Wound Care Fall 2020 meeting (SAWC; 4–6 November, online). Speaking in a session entitled “Oxygen and Healing: New Options”, Regulski presented positive results of his early experience using this therapy to treat perfusion-ischaemic wounds, and said he was “hopeful” that this would become a treatment used “from the get-go” in patients diagnosed as diabetic or pre-diabetic.
“Oxygen plays a big role in the healing process, and a lack of the essential element spells trouble,” the blurb for the SAWC session contextualises. “Remote ischaemic conditioning is one of the emerging technologies showing promise in treating chronic wound hypoxia.”
Showing a bar chart depicting relative five-year mortality rates of various diseases, including pancreatic cancer (97%), ischaemic ulcer (55%), and breast cancer (18%), Regulski related how nearly half (45%) of all unhealed neuropathic ulcers result in death within five years. “I think there is a multitude of problems that are affecting the diabetic population; it is a multi-factorial, multi-systemic problem that is occurring. Diabetes affects every system in the body, and the complications that it causes and the strife that it causes for people I know is quite disheartening. But I do not think much of the public understand the gravity of the situation we are dealing with,” he commented.
In addition to the high mortality rate—which increases substantially when diabetic ulcers are combined with peripheral vascular disease—Regulski also explained how complications associated with diabetic foot ulcers are more expensive than the five most-costly cancers (breast cancer, colorectal cancer, lung cancer, prostate cancer, and leukaemia), with a direct annual cost of US$17 billion a year.
Healing neuropathic ulcers is difficult. A meta-analysis published in Diabetes Care in 1999 found that, after 20 weeks of good wound care, approximately 31% of diabetic neuropathic ulcers heal. Twenty-four percent had healed after 12 weeks of good care. “That is not very good,” Regulski opined. “That is not very good at all. That is why we have moved into these new realms of innovative, advanced therapies.”
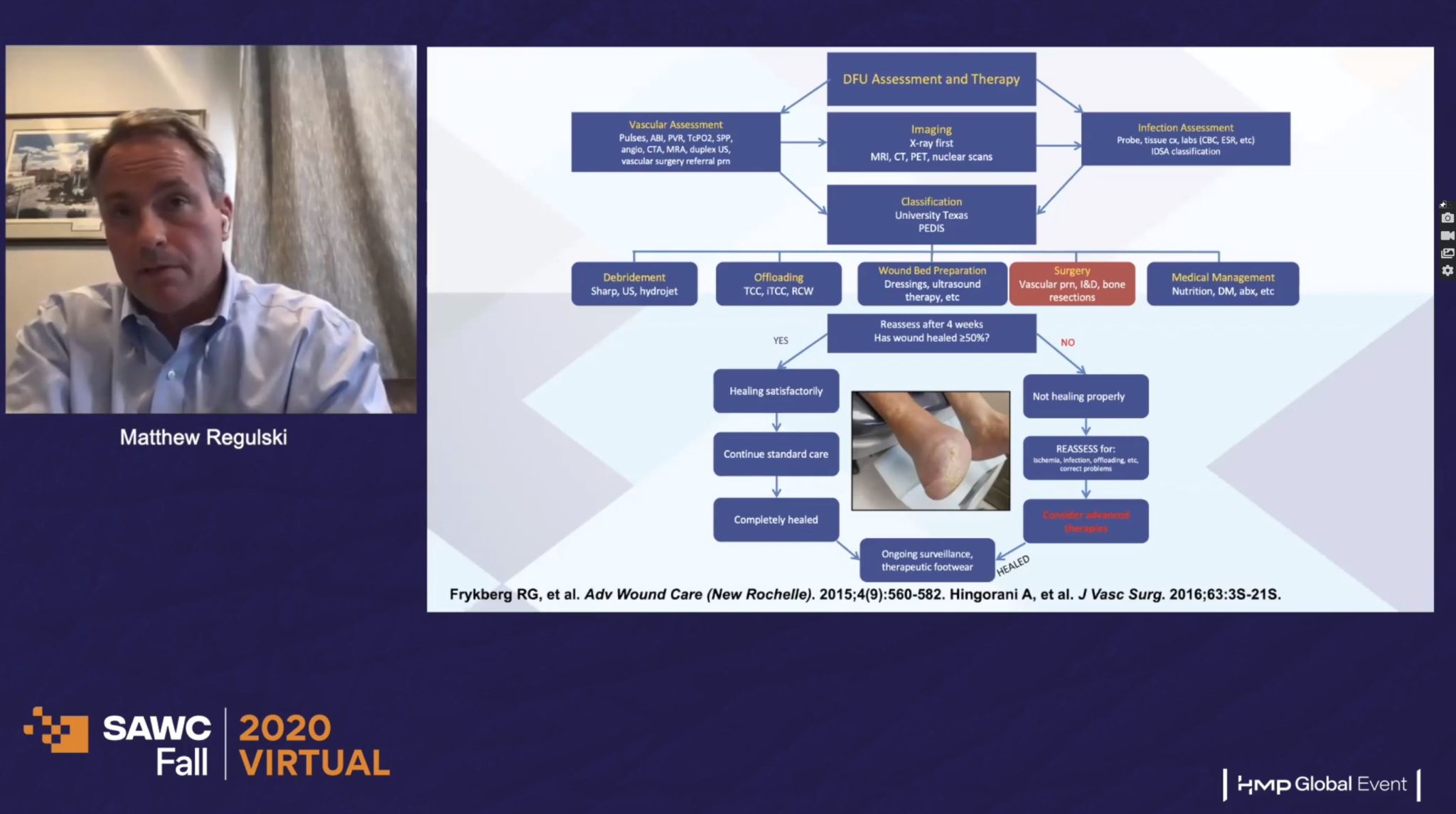
Against this backdrop, Regulski introduced remote ischaemic conditioning. If, four weeks after standard-of-care treatment—which could include debridement, offloading, wound bed preparation, surgery, and/or medical management— a patient’s diabetic foot ulcer wound has not healed by at least 50%, then the patient needs to be reassessed. It may be that a more advanced therapy should be considered.
Remote ischaemic conditioning, or tissue conditioning, involves the brief blocking of circulation in an arm or leg by applying pressure. It is an emerging treatment modality for reducing damage caused by ischaemia-reperfusion injury, and works by triggering an upregulation of the body’s anti-oxidant defence systems, which in turn help to dilute out inflammatory proteins and extinguish or mitigate the chronic inflammation occurring in the wound. It is administered by inflation of a pneumatic blood pressure cuff to a suprasystolic pressure on a limb.
“The conditioning is a very simple thing,” Regulski explained. “It is not a blood pressure cuff; I know people are going to think it is just a blood pressure cuff. It is a very proprietary development. [The technology] senses your blood pressure every 30 seconds, and then it goes a specific amount of mmHg above that—it has been figured out by people much smarter than I am what is the right amount of pressure to stimulate these signals and this cascade effect that is occurring in your body. It is really a fascinating thing. Compliance is incredibly high, because people can sit at home, watch TV (I have even had patients who are still smoking that are doing it!), and do this.”
A new clinical wave: The data for remote ischaemic conditioning in diabetic foot ulcers
“It is really interesting to see the capabilities remote ischaemic condition can have for a multitude of cardiovascular outcomes to prevent a lot of different problems that have been put forth in people who have cardiovascular disease,” Regulski said, noting that the cardiovascular arena is where most of the data for remote ischaemic conditioning use are from.
He informed delegates that the lack of large pivotal studies has delayed remote ischaemic conditioning adoption, but that three such studies “will open the door to broad-scale adoption”.
Speaking of the data for remote ischaemic conditioning, he said: “There have been some clinical trials that have been done on it in patients who have had stroke treatments, and to reduce heart attacks, to reduce fibrosis, and to reduce heart failure. Then we thought: ‘Well, if they have good results for that, is there a capability that we could use, could we upregulate the body’s systems and begin to heal these [patients] from the inside?’ It is a very daunting task, and there is a lot of science that goes into the development of this machine. Again, it is not just a blood pressure cuff that you are going to be using, but it is a very proprietary, patented technology.
“Our hope is that we will be able to have these types of devices in ambulances and in operating rooms that we can use on patients to mitigate these problems, and to help in part of that healing spectrum.”
Detailing the automated delivery of the treatment, Regulski informed his audience that it is easy to operate, needing no assembly and being a one-button device. Vital signs monitoring is included as part of the device, and it is fully disposable, meaning there is no MRSA risk, and no cleaning, recharge, or maintenance. It takes 40 minutes, three times a week.
Describing his experience of this technology, which is yet to be published, Regulski reported how he and his colleagues conducted a matched pair analysis: 46 wounds were matched for location and size at baseline; the median wound duration was 118 days at baseline, and all patients had failed standard-of-care treatment options. Patients then received remote ischaemic conditioning therapy three times a week for 12–20 weeks. Regulski used the Tissue Analytics app to take photos and record measurements of the patients’ wounds as the study progressed.
Mean wound size decreased each week when treated with remote ischaemic conditioning compared to their matched partner.
“I am always sceptical when trying new things,” he said, addressing his initial thoughts about remote ischaemic conditioning. “People talk about how good things can be, and I have had patients that have had terrible wounds for a very long time, have multiple co-morbidities, have been non-compliant, so I thought ‘Let us see how this goes in the real-world’. I included people on dialysis, people with very low ankle-brachial index scores (down to 0.6), because these are people not always included in normal clinical trial work. If this was going to work, I had to see how it did on these people, because these are the people that you and I are seeing every day.”
“I was pleasantly surprised by [our outcomes],” he concluded. “I was very thankful that I was able to be part of this, because I think this is going to be a very innovative therapy. Hopefully, we can use this right from the get-go when someone is diagnosed as diabetic or in the pre-diabetic stage, with hypertension, signs of vascular disease–this is something we can start using to mitigate these risk factors.
“To be able to sit at your house, avail yourself of this therapy, place this cuff around [your arm or leg], be able to turn it on, to be able to talk through it too to your clinician, so we can maintain the compliance aspect of it where the patient is safe and comfortable, it is really incredible.”
Regulski and colleagues are currently collecting secondary data on kidney function, skin perfusion, effects on the eye, and in the blood, specifically looking at signal cascades produced by remote ischaemic conditioning.








