DISRUPT BTK II results out to 12 months demonstrate the strong safety profile and consistent effectiveness of the Shockwave peripheral intravascular lithotripsy (IVL) system (J&J MedTech/Shockwave Medical) for the treatment of calcified lesions below the knee (BTK) in patients suffering with peripheral arterial disease (PAD). The new data were presented in a late-breaking presentation at the 2025 Vascular Interventional Advances (VIVA) conference (2–5 November, Las Vegas, USA).
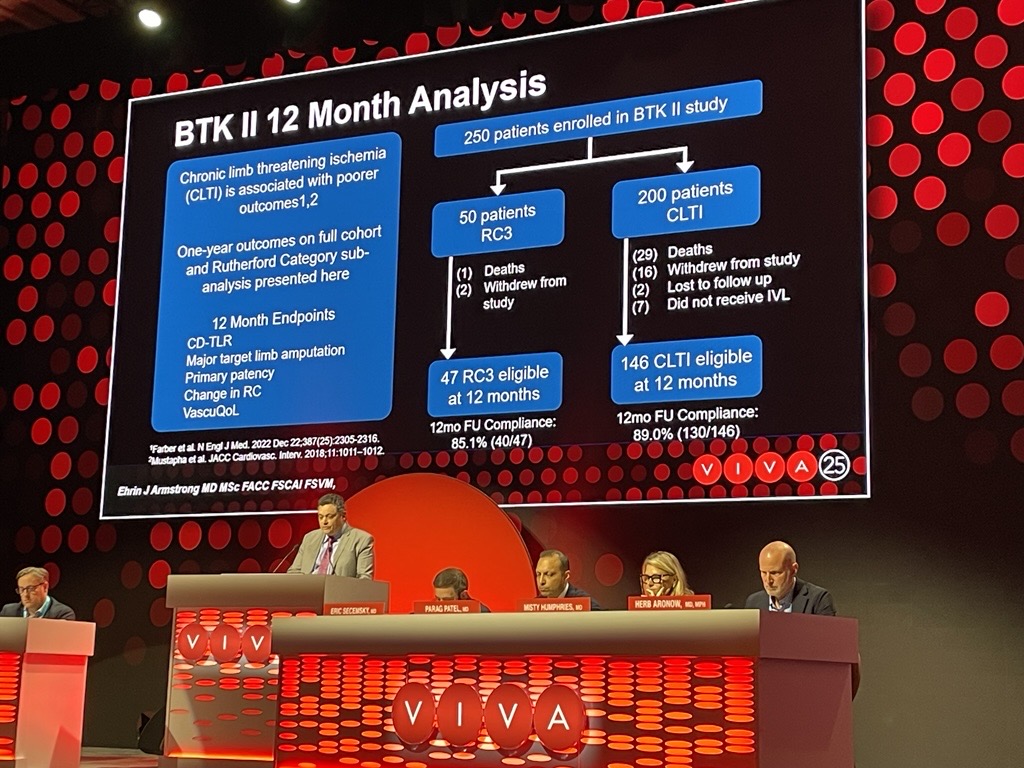
DISRUPT BTK II is a postmarket, prospective, multicentre, core lab-adjudicated, single-arm study that enrolled 250 patients with 305 lesions across 38 sites globally. In the study, 58.5% of patients presented with baseline wounds, 80% with chronic limb-threatening ischaemia (CLTI), 70% with diabetes mellitus, 30% with chronic total occlusions (CTOs), and 85% with moderate-to-severe calcium.
“Treating patients with complex BTK lesions has always been a major challenge with limited options available. DISRUPT BTK II sets a new standard by introducing IVL as a frontline strategy to modify calcification and restore vessel compliance for this high-risk patient population,” said Ehrin Armstrong (Swedish Medical Center, Denver, USA), who presented the data. “Shockwave IVL is one of the first technologies rigorously tested in severely calcified lesions, delivering low amputation rates and meaningful symptom relief—a major milestone in vascular care.”
Key findings from the full cohort at one year include:
- Freedom from major target limb amputation was achieved in 94.8% of patients at one year, with no amputations in non-CLTI patients.
- Freedom from clinically driven target revascularisation was achieved in 84.5% of patients at one year.
- Durable patency was observed in 67.1% of patients at one year.
- Rutherford Category (RC) class improvement was achieved in 75.5% of patients at one year. Patients improved from their baseline Rutherford class status by at least one class with nearly 50% rendered asymptomatic at one year. Additionally, wound healing or improvement was observed in 61.3% of patients.
Key findings within the CLTI cohort at one year, which comprised 80% of trial patients, include:
- In patients with CLTI at baseline, 8.1% had an amputation.
- The proportion of patients with a CLTI Rutherford classification improved from 80.1% at baseline to just 25.1% with available one-year follow-up.
- Significant symptomatic and VascuQoL improvements were documented with a more than five-point improvement from baseline (11.9±4 to 17.2±5, p<0.001) at one year.
- For patients with CLTI, 82.7% remained free from clinically driven target lesion revascularisation (CD-TLR) at one year.
- At one year, the primary patency rate was 64%.
“The DISRUPT BTK II study represents a complex, truly real-world patient and lesion cohort,” Armstrong said in his concluding remarks, noting high rates of diabetes mellitus, severe target lesion calcification, dialysis-dependent renal failure, and CLTI with wounds amongst the patient population.
He summarised the latest findings: “One-year results support the use of IVL in the treatment of this challenging patient population, with low rates of CD-TLR and amputation and significant symptomatic improvements.”










