This advertorial is sponsored by Bentley.
Complex peripheral chronic total occlusions (CTOs) represent a daily challenge for interventionalists, necessitating a standardised approach for optimal patient outcomes. A team of experts has developed such a protocol—published in 2023 in JACC: Cardiovascular Interventions. Interventional vascular specialist Andrej Schmidt (University Hospital Leipzig, Leipzig, Germany), one of the co-authors of the algorithm, has extensive experience in this field. The BeBack crossing and re-entry catheter is bringing a change to this algorithm in Schmidt’s practice, adding simplicity with its multitool function and giving the option to either stay intraluminal or go subintimal with a re-entry.
Integrating the BeBack before advanced techniques
Schmidt notes that his centre is one of the largest in Germany for the endovascular treatment of peripheral arterial occlusive disease and receives a high number of complex cases. He describes the BeBack as a “reliable” crossing and re-entry device for the treatment of such cases, noting its “slim yet stable” design.
Schmidt uses the device first and foremost as a crossing tool, and secondly as a bailout option for reentry when going subintimal. “We try harder now to stay intraluminal and BeBack is one of the tools that we use for that,” he states. For example, the device can be used in cases of calcified CTOs where wire passage with catheters and CTO wires will not work. While these are “really selected cases,” Schmidt says, they are becoming more common.
For long CTOs, especially if they are complex, calcified lesions, Schmidt remarks that it does not make sense to stay intraluminal. In these situations, he says, the BeBack can be used as a re-entry device.
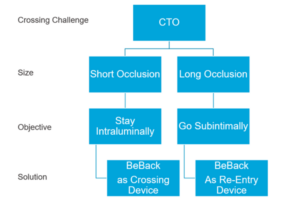 Summarising his approach, Schmidt shares the following guidance for using the BeBack prior to the advanced technique stage of the algorithm: for short occlusions, stay intraluminal and use it as a crossing device; for long occlusions, go subintimal and use it as a re-entry device.
Summarising his approach, Schmidt shares the following guidance for using the BeBack prior to the advanced technique stage of the algorithm: for short occlusions, stay intraluminal and use it as a crossing device; for long occlusions, go subintimal and use it as a re-entry device.
According to Schmidt, the algorithm can be expanded depending on the morphology and size of the occlusion in question, with the BeBack often coming into play. “Once you get into the situation where you have to go retrograde,” he says, “then the BeBack can be incorporated into a more detailed algorithm.”
Schmidt opines that the BeBack has changed the CTO crossing algorithm for the better, making interventions simpler, quicker, and more reliable. For example, Schmidt notes that the device is easier to use for re-entry than earlier options. As a result, he says, “it can be used in a much larger variety of cases”.
He continues that the device has shortened procedure times in the event of antegrade and retrograde failure. “If we cannot go through using either an antegrade or a retrograde approach, we can go directly to one balloon from one side and the BeBack from the other side,” he explains, comparing this to having to use two balloons when the device is not part of the procedure. In addition, due to the 4Fr size of the device, Schmidt details that it can be taken through tibial sheaths in complex retrograde-access cases, “which has made the intervention faster and more reliable”.
Listing the indications for the BeBack, Schmidt shares that he has used the device in superficial femoral artery (SFA), below-the-knee (BTK) and venous lesions, as well as intraluminally in the iliacs. On the latter, he comments: “With re-entry devices we hesitated in the past because in the iliacs we don’t want to puncture in the wrong direction. Using the BeBack we now feel more comfortable, because it’s slimmer than other re-entry devices.” He continues that using the device in this morphology makes for a “more elegant” procedure.
Schmidt has considerable experience using the BeBack in iliac arteries. In fact, his first experience with the device was during the treatment of a CTO of the common iliac artery in an abdominal aneurysm patient. “We failed to get through the CTO coming from retrograde, cross-over and antegrade using an arm-access,” he recalls. “Nothing worked, until eventually we used the BeBack catheter via the retrograde approach. With this, device passage through the CTO back into the aorta succeeded immediately. This experience was an eye-opener for us with regard to the success of this catheter.”
CTO crossing algorithm
In their 2023 JACC: Cardiovascular Interventions paper, Schmidt and colleagues set out a step-by-step guide to crossing CTOs.
- The authors first advise choosing an optimal access site, evaluating the CTO by computed tomography (CT) angiography, and evaluating the proximal/distal cap morphology and other angiographic parameters predicting feasibility of antegrade passage.
- As a next step, Schmidt et al suggest opting for an antegrade approach initially and then, in the event of antegrade failure, attempting retrograde access. The authors recommend changing strategy to an advanced technique and/or re-entry device in the event of failure of both antegrade and retrograde access.
- Subsequently, in the event of success, Schmidt et al encourage proceeding with either treatment from antegrade (if antegrade was used initially) or wire externalisation and treatment from antegrade (if retrograde was used initially). In the event of failure—specifically if no progress has been made after three hours or in the instance of high radiation or contrast dosage, patient discomfort or vessel-specific complications—the authors advise stopping the procedure and instead changing course to a conservative treatment strategy or planning either redo or open surgery.
“By establishing the algorithm in the daily routine of endovascular specialists, improvements in vessel and patientspecific outcomes are anticipated,” Schmidt et al write. The authors go on to state that “future research and continued collaboration between experts is warranted”.
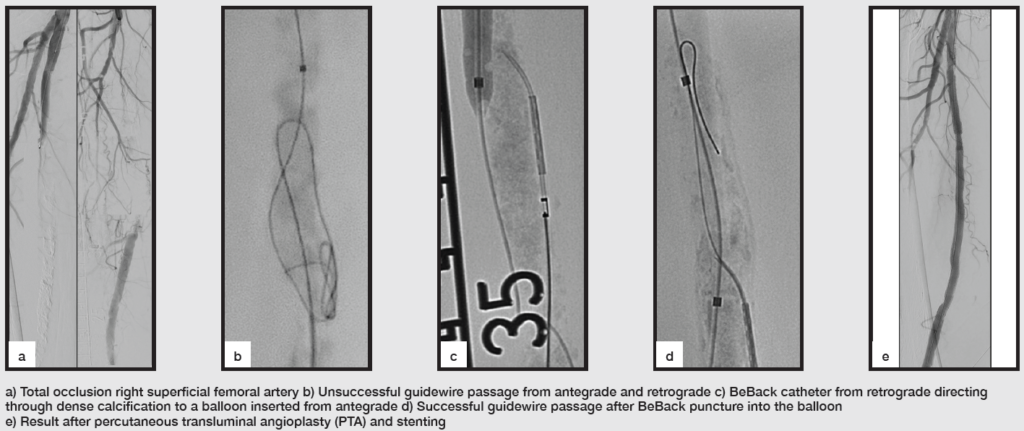
BeBack case images