This advertorial is sponsored by Bentley.

Stéphan Haulon (Hôpital Marie Lannelongue, GHPSJ, Paris, France) has extensive clinical experience using the BeGraft (Bentley, Hechingen, Germany) as a bridging stent in fenestrated endovascular aneurysm repair (FEVAR) procedures. He has conducted a pioneering study on the topic, with the latest published data pointing to excellent patency out to three years. In this interview, Haulon speaks to Vascular News about how the BeGraft has changed his approach to certain fenestrated procedures, outlines the key features of a good bridging stent and underscores how his dataset and others pave the way for an on-label indication for the BeGraft as a bridging stent in FEVAR procedures.
In what ways has the BeGraft as a bridging stent changed how you implant a fenestrated graft?
I think the BeGraft has changed our workflow and the ancillary tools that we are using. We have almost exclusively changed to using 6Fr catheters to get into the target vessel, whereas previously we were using 7Fr sheaths routinely. The access you need from the iliacs is smaller with a 6Fr catheter, especially when using a pre-loaded system. If you use a pre-loaded renal fenestrated endograft you can access both renal arteries from the side of the endograft delivery system, and then on the other side you only need to access the two visceral vessels. In cases such as this we can use a 14Fr sheath where we might once have used a 20Fr or larger sheath. It is risky to use large sheaths in the iliacs because they can cause rupture, and so if we can avoid using them that makes the procedure safer.
What are the main features of a good bridging stent?
I think you need to combine a good endograft design with a good bridging stent in order to achieve positive outcomes. In my experience, using endografts with the fenestration positioned at the origin of the target vessel—meaning that there is no gap between the origin of target vessel and the fenestration—provides a very stable platform for BeGraft as a bridging stent. In addition, the bridging stent needs to be 6Fr compatible so that you can easily and safely position it in the target vessel. It also needs to be flexible so that it can adapt to the various forces that are exerted on the target vessel. In the renal artery, for example, the first 20mm moves with the aorta and then the distal portion moves with respiratory motion, and so a flexible stent is really important here if you want to avoid issues during follow-up. Furthermore, it is necessary to have various diameters and lengths available so that you can adapt your approach to the patient anatomy and safely perform the procedure. With the BeGraft you have a lot of options available in this regard.

How does the BeGraft compare to other bridging stents on the market?
I think the BeGraft is very flexible, and the 200 microns thickness of the ePTFE provides a secure coverage of the cobalt-chromium stent. It is always difficult to compare stents, however, in my experience, the BeGraft is perfectly suited for use as a bridging stent in FEVAR and we now have strong data to support this.
You conducted a study with the BeGraft as a bridging stent in FEVAR. What were the endpoints?
We were looking primarily at the patency of fenestrated endografts for short necks or juxtarenal aneurysms. In addition, we were looking for things like type III endoleaks and stent fractures.
Three-year data from this study have been published. Could you briefly summarise the main outcomes at this time point?
The patency was excellent and there were only two secondary procedures. I think these outcomes are a result of good patient selection, sizing and graft design. If you design the appropriate fenestrated endograft, then the BeGraft will provide a perfect platform.
Furthermore, I think we had such a low number of technical issues because we perform a cone-beam computed tomography (CT) scan at the end of each procedure, and I think this should be routine. If you capture an issue at the end of the procedure with your cone-beam CT, you can fix it right away, and then you do not need a secondary procedure.
Will there be further follow-up of these patients?
All our patients are in a prospective cohort, and so we continue to collect data on these patients. We have been using the BeGraft as our primary bridging stent for around seven years now, and we have more than 500 fenestrated cases in our database. There is also a dedicated prospective study currently running in Germany to evaluate the BeGraft as a bridging stent for fenestrated endografts. It is great that data are coming from different centres to consolidate our findings.
You also performed a study on the movements of stents once they have been implanted. Could you outline the key findings from this study?
We know, and as mentioned in your previous question, that there is some movement in all the target vessels during respiratory motion. All patients enrolled in that study underwent a pre-operative CT scan in inspiratory and expiratory motion, and then we did the same scan postoperatively with the endograft and the BeGraft in all target vessels and performed again inspiratory and expiratory acquisition of the CT scan. We looked at how the bridging stent modified the way those visceral vessels behaved and it was very interesting to see that there was only a minimal impact. We were actually not changing the way those target vessels behave.
Bentley is working on an on-label indication for the BeGraft in FEVAR. Why now?
While it takes a lot of effort and a lot of financial commitment to get on-label approval, I think Bentley understood that it was time to undertake such a project. Moreover, physicians have been pushing for a dedicated bridging stent for a long time and working hard on compiling the data to support an on-label indication. In Europe, I think that very soon the BeGraft Peripheral will have an indication for FEVAR and the BeGraft Plus will soon have an indication for branched endovascular repair (BEVAR). To date we have all had to use the bridging stents in an off-label setting for FEVAR procedures, and so I and other physicians are very pleased that an on-label indication is on its way.
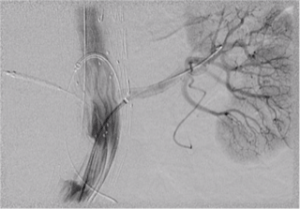
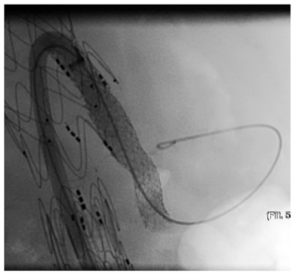
Case images: Selective angiograms confirming patency and sealing after implantation of a BeGraft into the left renal artery during FEVAR and into the coeliac trunk during BEVAR