 On the night of 13 November 2015, bombing and shooting attacks in Paris, France, killed 130 people and wounded another 352. The attacks—targeting a football match, a music venue and several bars and restaurants—were the deadliest in France since World War II and the deadliest in the European Union since the 2004 Madrid train bombings.
On the night of 13 November 2015, bombing and shooting attacks in Paris, France, killed 130 people and wounded another 352. The attacks—targeting a football match, a music venue and several bars and restaurants—were the deadliest in France since World War II and the deadliest in the European Union since the 2004 Madrid train bombings.
Guillaume Boddaert was part of the team at Percy Military Teaching Hospital, where 17 victims of the attacks were treated. He spoke to Vascular News about how his centre dealt with the attacks and how the centre has since adapted its mass casualty incident strategies based on lessons learned that night.
Can you tell us about Percy Military Teaching Hospital?
Percy Military Teaching Hospital is medium-sized level-1 trauma centre located near Paris. It has 300 beds including 14 general intensive care beds, 13 intensive care beds in a burn unit and seven operating rooms (ORs). On duty, there are three senior intensivists and one intern, one general surgeon (often a digestive specialist), one orthopaedic surgeon, one neurosurgeon and one maxillofacial surgeon. On call, there are personnel for thoracic surgery, vascular surgery and embolisation.
The main mission of Percy Military Teaching Hospital is to support the French military, and especially its member wounded while on deployment. Thus, our domain of excellence is the management of polytrauma patients and ballistic wounds. However, our hospital is open to everyone, including civilian patients, and offers numerous qualified medicine departments.
On the night of the attacks how did the hospital prepare for casualties to arrive?
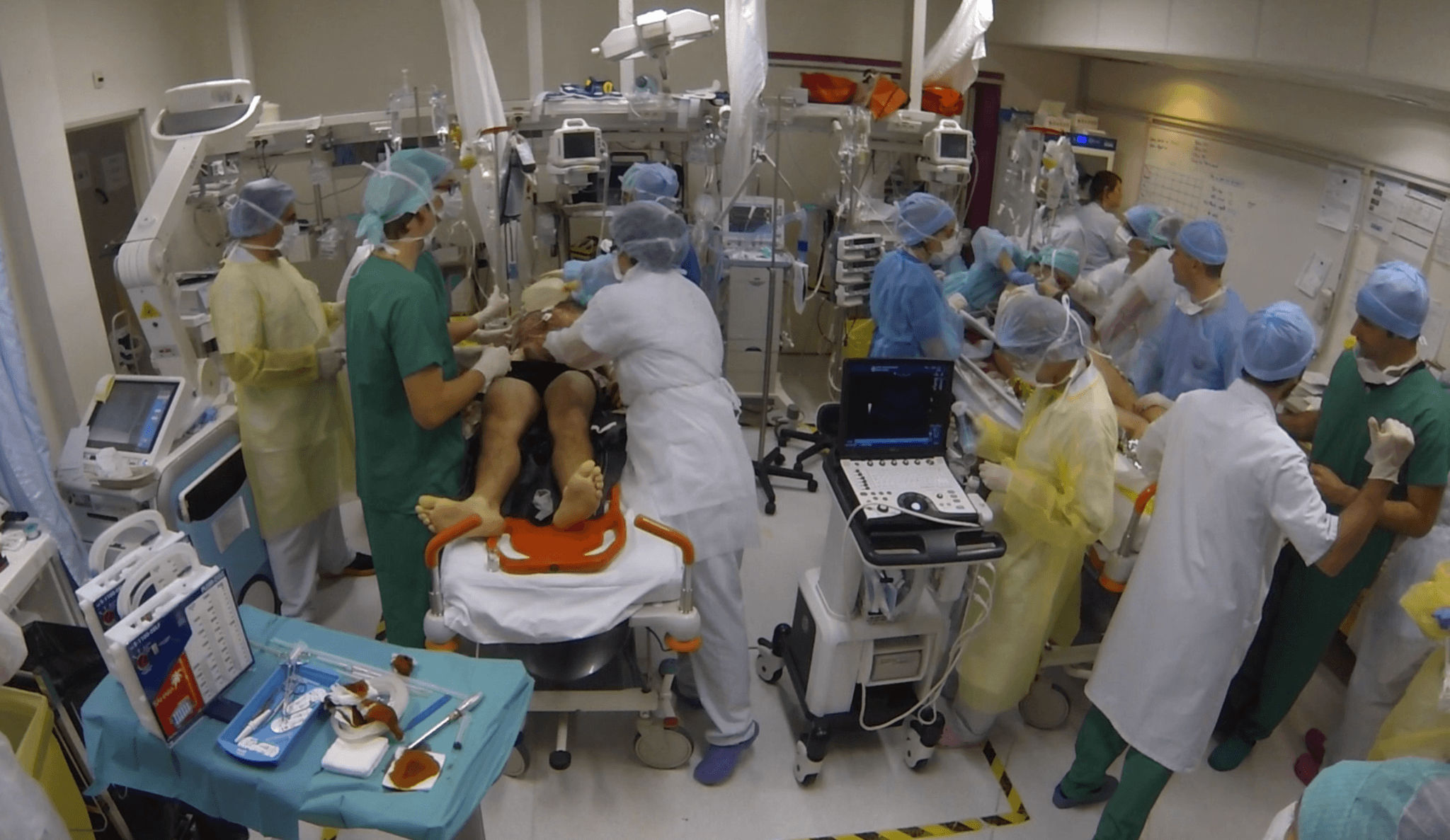
The emergency alert began at 9:45pm. Immediately, we set up a crisis unit, activated the mass casualty incident protocol, called back staff, and cleared the emergency department, ORs, post-anaesthesia care unit (PACU) and intensive care units (ICUs). We were able to accept five absolute emergencies and 13 relative emergencies. Six operating rooms were prepared, and we also activated computed tomography (CT), embolisation, the blood bank, the sterilisation and a psychological cell. We also set-up a triage cross, as we do in deployment, according to the “walking forward principle”. The first wave of patients arrived at 11:55pm. Numerical temporary identities were systematically assigned to patients at the entrance and they were directed either to the absolute emergency or relative emergency areas, or directly to the OR as was the case for one patient. All patient information was written on a large white triage board, allowing the staff to follow all the patients.
How were patients processed and prioritised?
Pre-hospital admittance categorisation was reported as absolute emergency or relative emergency according to the pre-hospital admittance rescue organisation plan called the “Red Plan” (Plan Rouge). Absolute emergencies require surgery or embolisation without delay, whereas relative emergencies may be managed secondarily.
In-hospital triage was binomial, involving an intensivist and a surgeon. Categorisation was reported as immediate (T1), delayed (T2), minimal (T3) or expectant (T4) according to French and NATO Military Health Service recommendations.
In the immediate group are casualties who required attention within two hours on arrival to avoid death or major disability. The delayed group include those wounded and in need of surgery, but whose general condition permits delay in treatment without unduly endangering life, limb, or eyesight. The minimal group consists of those patients who have relatively minor injuries and can effectively care for themselves or be treated with minimal medical care. Patients in the expectant group are casualties that would overwhelm available medical resources at the expense of treating salvageable patients.

How different were the injuries on this night compared with your usual patients?
In France, ballistic wounds are relatively rare; we only manage this kind of trauma once a month. However, because of the nature of our hospital, our teams have learned to manage such casualties during recent conflicts in Afghanistan or in Sahel. Our teams are trained to handle war-wounded inflows in austere conditions and to manage saturating situations.
Generally, gunshot wound characteristics depend on the type of projectile, its velocity, encountering an obstacle, the distance, the position of the target and the type of injured organs. There are four components of projectile wounding. The first is depth penetration. The second is the permanent cavity, which is the volume of tissues destroyed by the passage of the projectile. The narrow portion at the start of the permanent cavity is called the “neck”. Following this neck, high projectiles may destabilise and tumble, leading to hazardous trajectories. The third is the temporary cavity, which corresponds to the stretching of the permanent cavity due to the transfer of kinetic energy during the passage of the projectile. The fourth is the fragmentation of the projectile or bones, which are dispersed outward from the permanent cavity, potentially causing additional tissue damage.
During the Paris attacks, the patients were victims of high-velocity gunshot wounds and, contrary to soldiers in deployment, were not protected. This resulted in high-grade injuries, especially of the trunk, with multi-cavity wounds requiring multidisciplinary management. However, whatever the lesions, we systematically applied trauma management standards and damage control principles.
How did you ensure that facilities were available for patients arriving throughout the night?
Throughout the alert, we adopted a systematic damage control strategy to rapidly release operating room rooms and treat as many patients as possible. A definitive surgical treatment was done thereafter at 48 hours.
Damage control surgery (DCS) is a shortened surgery, limited to 60 minutes. Procedures are temporary and aim to achieve haemostasis, aerostasis and coprostasis, without closing the patient definitively. The philosophy is to prioritise physiology and homeostasis, to the detriment of an exhaustive anatomical repair, ad integrum, which can be deleterious in patients with high traumatic load.
The second stage is resuscitation, the objective of which is the correction of physiological disorders, essentially coagulopathy-acidosis-hypothermia. Finally, the third stage is performed between 24 and 48 hours once the patient is stabilised, and aims to achieve definitive surgical repair.
The indications for DCS are individual and collective. The individual indications are related to the physiological status of the patient and/or the complexity of the procedure. The aim is to avoid patient exhaustion and multiple organ dysfunction syndrome. From a collective point of view, the aim is to prevent a saturating situation and to be able to manage the maximum number of patients in the minimum time.
Before the attacks, how often did your hospital practise for emergencies like this one?
We have a working group on trauma in our hospital. This group is in charge of communication, teaching, development of the procedures and protocols, practice assessment and, finally, our trauma base. Twice a year, we organise two days of trauma patient simulation. Four scenarios are simulated, one of which may be a mass casualties incident.
Besides, as mentioned, our teams have faced war-wounded inflows in saturating conditions during recent conflicts in Afghanistan, Sahel or the Central African Republic; they have learned to manage such situations.
Fortunately, during the Paris attacks, we were not in a saturating situation. We only treated 17 patients and would have probably been able to do more if necessary.
Wartime in-hospital triage and damage control strategies have significantly contributed to the fluidity of patient management during these events. However, some other points have to be underlined. First, these attacks happened on a Friday evening and all ORs, except one, were free; it would have been more complicated on a busy weekday.
Second, the first wave of wounded patients arrived almost two hours after the alert, so we had time to get prepared. This probably would have been different if we had been closer to the events and if the patients had arrived earlier, as happened in some other hospitals.
Another crucial point is the systematic attribution of provisory identities as patient arrived, which allowed us to avoid errors.
Finally, I would like to mention the dual-command concept. A first cell of command is in the emergency department, is in charge of the triage and the orientation of the patients, and is in contact with pre-hospital regulation. The second cell is in the operating theatre and supervises surgical strategy and resources used, according to the information from the first cell.
What lessons did your hospital learn from this experience?
The first lesson is probably to remain humble. On this night, we were not saturated and thus were fully able to treat all of the patients we received.
We have reviewed all the medical records and the only death has been considered as unpreventable. However, some points of discussion have been highlighted and we may have faced problems if we have had to maintain the same level of activity for longer. The first is the absence of a real procedure for medical team recall and turnover. The second is the number of surgical instrument sets, especially visceral and thoracic, the sterilisation time for which is incompressible. Third is the stock depletion of some consumables (including chest tubes and negative pressure wound therapy systems, in particular). Finally, we noticed some difficulties in the traceability of blood products. Addressing these points, we have rewritten and made some slight changes to our mass casualty incident plan.
What advice can you give to other hospitals that are creating strategies for similar situations?
The current context exposes us to the threat of new possible terrorist attacks and requires that the medical community is prepared for the management of multiple war casualties. The familiarisation to the modern principles of war surgery now seems mandatory to face this type of situation.
I would like to salute the strength and the determination of all the healthcare professionals committed to patient care during the 13 November Paris attacks, and we pay homage to the patients and their relatives.










