
Based on the Janet Powell Honorary Lecture she gave at this year’s European Society for Vascular Surgery annual meeting (ESVS Month; 29 September–29 October, virtual), Rebecka Hultgren details contemporary knowledge within the broad spectrum of aortic diseases, with specific emphasis on relevant sex differences.
One can identify three areas that probably hold the largest gains in order to achieve a promising future for patients with aortic disease: first, to decrease aortic-disease related deaths in the population; secondly, to decrease aortic-disease related short-term deaths in the treated diagnosed population; and finally, to improve the long-term survival in successfully treated patients. An important factor to consider in all the efforts to achieve improved survival in the population is that the majority of persons, that also have an earlier onset of disease, are male. The women with an aortic disease represent a minority with a considerably later onset of disease. The primary focus has in the last three decades been to screen risk groups in the population with a high prevalence of disease. This has been evaluated and proven in elderly men in the well-cited randomised controlled trials (RCTs) and confirmed in later years in several observational studies. The only other possible screening model that could be cost-effective, also including women, would be to screen first-degree relatives to abdominal aortic aneurysm (AAA) patients, but these models must be evaluated further.
A more intriguing scientific challenge would be to further explore the triggers for development of disease in the population, in women and men, in order to minimise these risks. Ongoing translational work, animal models, and some clinical studies do support that sex hormones can be of great interest in this context. The immediate clinical value of such an understanding, of the possible causality between sex hormone levels and development of AAA presently is distant, but once this is explored or confirmed it will certainly influence our care trajectories of persons at risk.
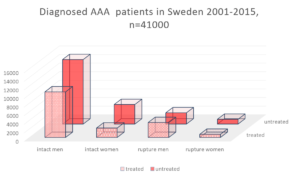
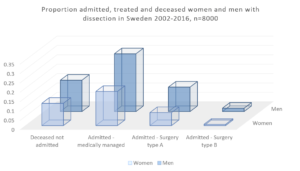
A problematic, important, and commonly ignored fact within this area is that the vast majority of patients with aortic disease never are treated, and this large proportion are not included in scientific work. The worse survival rate in treated groups of women with AAA has been shown repeatedly in many papers, for open, endovascular, intact or ruptured, or for complex aortic repair. This is unfortunately also now reported for other aortic disease groups, such as thoracic aortic aneurysm (TAA) and dissection. To better understand the treated patients, and the dominating sex-differences in eligibility for treatment and worse outcome, this must be increasingly included in our scientific work. The histograms illustrate the Swedish experience with AAA patients and patients with dissection, visualised by showing the proportion of treated versus untreated patients with diagnosis. Women are repeatedly reported to be overrepresented in non-eligibility groups, untreated at rupture or in intact AAA cohorts, with few in-depth explorations to investigate such sex-or gender differences. To move the understanding of eligibility and treatment outcome forward in clinical care, one must include new perspectives on how we survey patients and what the thresholds for repair actually are based on. The concept of aortic size index (ASI), rather than just diameter will certainly be included in the future models of surveillance strategies. Other methods that could certify that patients are treated “just-in-time” are possible complimentary biomechanical methods. It is sad to note that we still, even if the knowledge of ASI and biomechanic methodology has been out there for quite some years, still do not have the means to include it in daily clinical practice. Possibly RCTs are the only way to move in order to include it in future recommendations.
Last, the poor long-term relative survival in treated AAA patients was reported quite some years ago from us and others. This was recently confirmed again in a new collaborative project with The Netherlands, a manifest 20% lower relative survival at four years for treated women, even when compared to a population with similar risk factors. This is an area where we would have expected improvement over time, with improved secondary prevention strategies, but unfortunately, no real positive trend is found for men or women.
The future could be promising for all patients within the whole spectrum of aortic diseases, but care-givers in vascular surgery must improve their understanding of clinically relevant sex or gender differences by combining knowledge from guidelines, clinical and translational papers, and exploring their national-regional outcomes with these perspectives in order to achieve this goal. A more robust clinical implementation of our broad scientific knowledge will change the future for our aortic patients, both women and men.
Selected references from the lecture
- Bulder, R, Talvitie M, Hultgren R, et al. Long-term prognosis after elective AAA is poor in women and men: the challenges remain. Annals of Surgery, in press, 2020, PMID: 32657926.
- Smedberg C, Steuer J, Leander K, Hultgren R. Incidence, time trends and sex differences in aortic dissection: a population based study on Swedish patients during 15 years. European Heart Journal, Volume 41, Issue 26, Pages 2430–2438 e-pub June 2020.
- Ulug P, Sweeting MJ, von Allmen RS, et al. Morphological suitability for endovascular repair, non-intervention rates, and operative mortality in women and men assessed for intact abdominal aortic aneurysm repair: systematic reviews with meta-analysis. Lancet 2017 Jun 24;389(10088):2482–2491. doi: 10.1016/S0140–6736(17)30639-6. PMID: 28455148 Review.
- Wanhainen A, Verzini F, Van Herzeele I, et al. Editor’s Choice – European Society for Vascular Surgery (ESVS) 2019 Clinical Practice Guidelines on the Management of Abdominal Aorto-iliac Artery Aneurysms. European Journal of Vascular and Endovascular Surgery 2019 Jan;57(1):8–93. doi: 10.1016/j.ejvs.2018.09.020, PMID: 30528142.
- Sakahalisan N, Defraigne J, Katsargyris A, et al. Abdominal Aortic Aneurysms. Nature Reviews Disease Primers 2018 Vol 4:1 34.
- Lo RC, Lu B, Fokkema MT, et al. Relative importance of aneurysm diameter and body size for predicting abdominal aortic aneurysm rupture in men and women. Journal of Vascular Surgery 2014 May;59(5):1209–16. doi: 10.1016/j.jvs.2013.10.104. Epub 2013 Dec 30.PMID: 24388278.
- Hultgren R, Linne A, Svensjö S. Cost effectiveness of targeted screening of siblings to individuals with abdominal aortic aneurysms. British Journal of Surgery 2019 Feb;106(3):206–216. doi: 10.1002/ bjs.11047. PMID:30702746.
- Villard C and Hultgren R. Abdominal aortic aneurysm – sex differences. Maturitas e-pub January, April 2018, 109, p 63–69.
- Zommorodi, Bottai and Hultgren. Sex differences in repair rates and outcome in patients with ruptured abdominal aortic aneurysm – a nationwide propensity-score-matched analysis of 10,724 patients. e-published British Journal of Surgery 2019 Oct;106(11):1480–1487. PMID 31403186.
- Fattahi, Rosenblad, Kragsterman, et al. Risk factors in 50-year-old men predicting development of abdominal aortic aneurysm – a prospective cohort study with 15 years of follow-up. Journal of Vascular Surgery 2020 Febr 27, PMID 32115319.
- Hultgren, Elfström, Öhman, et al. Six-year follow up in men invited to a population-based abdominal aortic aneurysm screening program. Angiology, volume 71 Issue 7, 641–649 e-pub 2020.
- Ulug P, Powell JT, Warschkow R, et al. Sex specific differences in the management of descending thoracic aortic aneurysms: systematic review with meta-analysis. European Journal of Vascular and Endovascular Surgery 2019 Oct;58(4):503–511. doi: 10.1016/j.ejvs.2019.04.022.
- Thompson SG, Bown MJ, Glover MJ, et al. Screening women aged 65 years or over for abdominal aortic aneurysm: a modelling study and health economic evaluation. Health Technol Assess 2018 Aug;22(43):1–142. doi: 10.3310/hta22430. PMID: 30132754.
Rebecka Hultgren is an adjunct professor at Karolinska Institutet and senior consultant in the Department of Vascular Surgery at Karolinska University Hospital (Stockholm, Sweden).
The author has no disclosures.











