According to the World Health Organization, around 300 million people are affected by the pathological oedema of limbs. Lymphoedema is caused by partial or total obstruction of lymphatic collectors as a consequence of skin and deep soft tissue inflammation, trauma of soft tissues and bones, lymphadenectomy and radiation in cancer therapy.
Effective treatment of such a large population has been a challenge for centuries. Moreover, none of the conservative and surgical methods so far applied have proved their ability to restore normal shape and function of limbs. Physiotherapy is the therapy of choice as a main modality or as a supplementary treatment to one of two surgical treatments: bridging drainage or excisional techniques. The microsurgical operations can be performed if some parts of the peripheral collecting lymphatics remain patent and partially drain oedematous regions. However, in advanced cases of lymphoedema, all main lymphatics are obstructed and tissue fluid accumulates in the interstitial spaces, spontaneously forming “blind channels” or “lakes”. The only solution in these cases would be to drain the spaces by creating artificial pathways for oedema fluid flow away to the non-obstructed regions where absorption of fluid can take place. This can be achieved by the formation of artificial pathways for oedema fluid flow in the shape of subcutaneous implantation of silicone tubing “lymphatics”, placed along the limb from the most distal part to its root, continuing to more proximal regions with fluid absorption capacity. In lower limbs this is an implant from the foot to the hypogastrium or lumbar region, and in upper limbs from the hand dorsum to the scapular area.
A 2cm-long incision is made in the hypogastrium or lumbar region 10cm above the inguinal crease or scapular area. A 1.5cm-wide and 100cm-long metal tunneler is introduced under the skin and bluntly moved in the subcutaneous tissue toward the thigh and internal aspect of the calf or forearm and hand dorsum. Other 2cm-long incisions are made in the groin, calf or forearm and the lower end of the conductor is exteriorised. Three silicone tubings with lateral holes at 5cm distance each are introduced into the lumen and moved upwards, after which the tunneler is removed. No fixing of tubings is necessary.
Silicone is hydrophobic and therefore there is no adhesion or ingrowth of tissue cells. Moreover, the elasticity of silicone prevents kinking, twisting or obstruction of the lumen. Before implantation, patients receive 1g of amoxicillin for one month and this is continued postoperatively for another month. After this, long-lasting penicillin is administered every three weeks for as long as tubings remain in the limb. This is now a routine procedure in prevention of dermato-lymphangio-adenitis (previously known as cellulitis). This low dose of antibiotic controls growth of bacteria normally present in lymph, especially in the presence of a foreign body. Patients are put on daily one-hour intermittent pneumatic compression for 14 days in the outpatient department and then at home. Elastic stockings with a second degree of compression are used before surgery. Limb circumference measurements are taken at five levels daily for the first 14 days in the outpatient department, and then weekly at home at the same time of the day and same limb position.


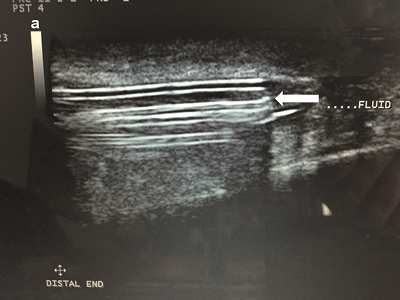
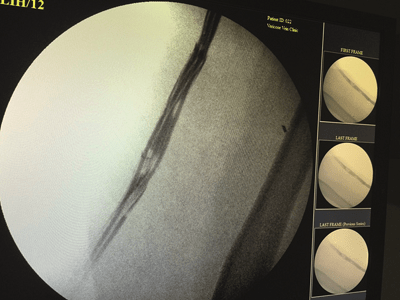
So far, 80 patients divided into two groups with lymphoedema of lower (50) limbs after hysterectomy and upper (30) limbs after mastectomy stage II and III have undergone implantation of silicone. Follow-up of 15 patients has almost reached four years. A rapid decrease in limb circumference was observed during the first days after implantation lasting for two weeks, which slowed thereafter. The mean decrease in circumference in mid-calf was 4% with range of 3 to 17%, in the forearm 10%, and 5% in the mid-arm during week one to reach 15 and 10% after four months, respectively (p<0.05). Patent tubings were seen on lymphoscintigraphy (Figures 1, 2 and 3) and accumulation of fluid on ultrasound images (Figure 4).
The accumulating tissue fluid cannot flow along the tubings by itself and requires a propelling force. This can be provided by the application of intermittent pneumatic compression as well as by having the patient walk in short stretch bandages or stockings. Tissue oedema fluid is drained from the swollen tissues to hypogastrium, lumbar or scapular regions. The question remains as to the absorption capacity of healthy tissues at the outlet of tubings. We observed a low degree of oedema developing in this region during the day activities subsiding during rest at night. This could be accounted for by sufficient absorption capacity from the hypogastrium.
There were no major inflammatory reactions to the implanted tubing in 95% of observed patients. In four patients an inflammation lasting for several days was seen in the leg at the upper end of implants and was easily controlled by antibiotics. This reaction was most likely caused by the microbes drained from the foot of the lymphoedematous limb. Under normal conditions single bacterial cells are transported from skin surface via lymphatics to the regional lymph nodes. Similar processes should take place along the implants. This cannot be considered as infection in clinical terms but rather as a physiological process of elimination of microbes by the lymphatic system.
Taken together, this study showed:
- Evident rapid decrease of calf circumference from the day of implantation and stabilisation when excess fluid was evacuated;
- Patency of tubings on ultrasonography and lymphoscintigraphy;
- Accumulation of fluid around the tubings in all cases;
- Lack of tissue cellular reaction to silicone tubings.
The simplicity of the surgical procedure and lack of reaction to the implant make the method worth applying in advanced stages of lymphoedema with large volumes of accumulated tissue fluid, preventing progression of anatomical changes specific for lymphoedema as fibrosis, hyperkeratosis and tissue fluid leakage.
Waldemar L Olszewski and Marzanna Zaleska are at the Medical Research Center, Polish Academy of Sciences and Central Clinical Hospital, Ministry of Home Affairs, Warsaw, Poland
References
Olszewski WL, Zaleska M. J Vasc Surg Venous Lymphatic 2015: (4); 401–408
Olszewski WL, Zaleska M. Int Angiol 2015 [Epub ahead of print]











