
The VasoStat (Forge Medical) is a haemostasis device designed for radial, brachial and transpedal procedures. The device is placed over the puncture site to achieve haemostasis by maintaining precise alignment over the radial artery across the needed range of pressure, without causing complete occlusion. Vascular News spoke to Timothy WI Clark, director of Interventional Radiology at Penn Presbyterian Medical Center, Philadelphia, USA, cofounder and chief executive officer of Forge Medical, about how the VasoStat was conceived and the clinical experience with the device so far.
What is the VasoStat device?
The use of radial access for coronary and peripheral interventions has been rapidly growing in the USA, and within the next five years is expected to approach rates seen in many parts of Europe, Canada, and Asia. In those and many other regions, radial access has supplanted femoral access as the dominant vascular access technique for most coronary and many peripheral (such as visceral embolisation) procedures. Brachial access continues to be widely used for a variety of niche applications, including complex endovascular aneurysm repair. Increasing numbers of patients with critical limb ischaemia has resulted in wider use of transpedal access during lower extremity revascularisation procedures, both for crossing/rendezvous techniques and even standalone access. The VasoStat is designed to have the versatility of achieving haemostasis in each of these anatomic locations. From a regulatory standpoint, the device has US Food and Drug Administration clearance and CE mark for upper extremity and pedal/tibial arterial puncture site haemostasis.
How did you first conceive of the VasoStat device?
Relatively long times to achieve haemostasis are seen following radial procedures. This has been attributed to the fact that the arteriotomy and sheath are substantially larger proportional to the size of the access artery compared to femoral access. What our practice has observed in the last decade of performing radial and transpedal procedures is that the most effective haemostasis can be obtained with highly focused pressure precisely aligned over the arteriotomy site, similar to holding a thumb or finger over the radial artery for the required length of time for successful haemostasis. Holding manual pressure for one to two hours is simply not feasible in a busy clinical environment, so an array of dedicated radial haemostasis devices have been introduced to the market. Current radial compression devices typically consist of one or more inflatable bladders tightly opposed to the arterial access site with a circumferential band encircling the wrist and fixated with overlapping Velcro. As the bladders are progressively inflated, greater compressive force is achieved over the volar aspect of the wrist. These balloon-type radial bands do not provide a high degree of precision and can be very uncomfortable for patients. Because of their lack of precision, longer times to haemostasis are required and a variety of complications have been observed, including arterial occlusion, nerve injury, venous congestion and skin injuries, ie. “handcuff syndrome”. We saw an unmet need for a different type of radial haemostasis device, and ideally one that could also be used for brachial and transpedal haemostasis.

We took an entirely different approach with the design of the VasoStat by emulating the physics of a human thumb or finger holding precise pressure aligned over the radial artery with the necessary amount of force based on the patient’s body habitus, residual heparin activity and sheath size. The VasoStat device consists of a central compressive plunger (similar to a person’s finger or thumb) which is aligned and anchored within an outer footplate. A unique ratcheting mechanism allows the operator to precisely control the degree of compression in a uniform fashion according to the needs of the individual patient. When sufficient time has elapsed to achieve haemostasis, the ratcheting mechanism is released to uncouple the compressive plunger from the footplate. The device is then peeled off the patient’s skin to remove it.
What are other differentiating features of the VasoStat?
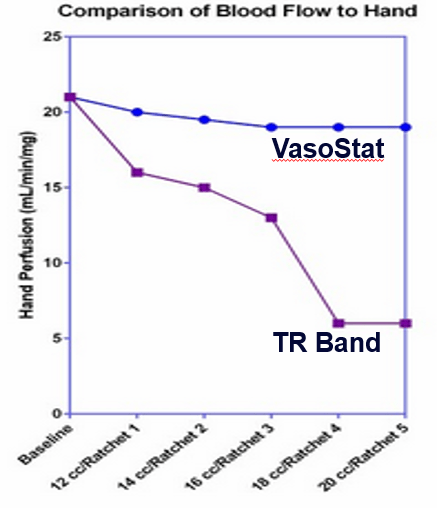 One significant concern of the balloon-type radial bands, which has never been really addressed in any of the existing literature to date, is that these devices occlude not only the radial artery, but also the ulnar artery. As a result, a marked reduction in hand perfusion occurs within the range of balloon inflation during clinical use. In a study performed at an independent facility using laser speckle imaging (which precisely quantitates hand perfusion), a 75% reduction in hand perfusion was seen with a band-type compression device. In contrast, the VasoStat device produced less than 9% reduction in normal hand perfusion within the range of clinical use.
One significant concern of the balloon-type radial bands, which has never been really addressed in any of the existing literature to date, is that these devices occlude not only the radial artery, but also the ulnar artery. As a result, a marked reduction in hand perfusion occurs within the range of balloon inflation during clinical use. In a study performed at an independent facility using laser speckle imaging (which precisely quantitates hand perfusion), a 75% reduction in hand perfusion was seen with a band-type compression device. In contrast, the VasoStat device produced less than 9% reduction in normal hand perfusion within the range of clinical use.

What is the clinical experience of the VasoStat device?
Though the Vasostat is a relatively new device, it has been used in the USA and Japan and has now also has CE mark.
In the USA, we are now just starting to see published outcomes with encouraging data on very low rates of access artery occlusion and other complications, while achieving haemostasis in substantially shorter times than balloon-type radial bands. In a study from our own centre at the University of Pennsylvania, in a cohort of patients undergoing a total of 72 radial, brachial, ulnar and transpedal interventions during embolisation or revascularisation procedures, VasoStat achieved successful haemostasis in 100% of cases. VasoStat produced substantially shorter times to haemostasis compared with previous studies employing balloon-type radial bands. The median time haemostasis in upper extremity access was just over 20 minutes, and the median time haemostasis following transpedal intervention was just over 40 minutes, which was attributed to heparin doses being double in the lower extremity access group. Only a single event of radial artery occlusion (1/72, 1.7%) was seen, which, although symptomatic, was successfully managed with mechanical thrombectomy. This study will be presented in more detail at the Society of Interventional Radiology meeting in March 2017.
In another study of 314 patients with Rutherford class 2–5 disease undergoing transpedal revascularisation, Kwan et al compared the performance of the VasoStat device with the TR Band (Terumo). Both devices showed equivalent performance in terms of time to haemostasis and a low rate of complications. However, the two groups were quite dissimilar in that almost all of the patients in the VasoStat group underwent complex, multilevel orbital atherectomy and angioplasty compared to simple balloon angioplasty in the majority of the TR Band group. Mean access artery diameter was also significantly smaller in the VasoStat group than the TR Band group. VasoStat substantially improved clinic workflow through a reduction in puncture site assessments and a streamlined removal protocol by nursing personnel, which enabled more cases to be performed on busy clinical days. We were very encouraged by these findings in that they showed VasoStat could be used safely and effectively in even complex transpedal intervention procedures entailing high doses of heparin. We have seen the biggest surge in the demand for VasoStat in the Japanese market. In Japan, hospitals are adopting VasoStat due to an improvement in catheterisation lab workflow compared to using balloon-type radial bands. We hope to see some outcomes and workflow efficiency data from high-volume Japanese hospitals soon.
What other studies are you anticipating with VasoStat?
The published experience to date has been retrospective. An investigator-initiated randomised controlled trial is currently underway in the USA among patients undergoing percutaneous coronary intervention (PCI) where haemostasis is achieved with the VasoStat haemostasis device versus a balloon-type radial band. It is too soon to comment on the results, although the preliminary data have been trending towards shorter times to haemostasis and a reduction in rebleeding events, further supporting the paradigm that precise focused pressure is critical to successful and time-efficient haemostasis in smaller vessels like the radial and pedal arteries. The design of the VasoStat device also makes it possible to combine it with physician-specified haemostatic agents that accelerate the coagulation cascade. This off-label use is something we have observed being performed by some high-volume practitioners, who report an even more dramatic reduction in time to haemostasis.
References
Kwan TW, Patel A, Parikh P et al. J Interven Cardiol 2016;29:424–430.
Uhlemann M, Möbius-Winkler S, Mende M et al. J Am Coll Cardiol Intv 2012;5:36–43.
Garg N, Madan BK, Khanna R, et al. J Invasive Cardiol 2015; 27(2):106–112.









